Localization of the genicular arteries under ultrasound guidance
- Affiliations
-
- 1Department of Anesthesiology and Pain Meidcine, Hanyang University Seoul Hospital, Seoul, Korea. jcshim@hanyang.ac.kr
- KMID: 2434202
- DOI: http://doi.org/10.17085/apm.2019.14.1.67
Abstract
- BACKGROUND
The genicular arteries (GAs) can be utilized for genicular nerve block. We aimed to evaluate the ability to localize GAs under ultrasound in patients with chronic knee pain.
METHODS
Twenty-four knees from 14 osteoarthritic patients were enrolled. The target GAs included the superomedial GA (SMGA), superolateral GA (SLGA), and inferomedial GA (IMGA). GAs were observed at the relevant adductor tubercle and epicondyle-shaft transition under ultrasound. Distribution of the SMGA at the adductor tubercle was evaluated using defined zones in transverse and longitudinal ultrasound images. SLGA and IMGA were also categorized using defined zones in longitudinal images. Distance from bony cortex to the relevant GA was then estimated.
RESULTS
Among 24 knees, 91.7% of SMGAs were located at the upper part of the adductor tubercle. The distances between the SMGA and bony cortex on transverse view (dSMGAt) and on longitudinal view (dSMGAl) were directly correlated (rs = 0.6539, P = 0.0005).
CONCLUSIONS
Under ultrasound guidance, the SMGA was found to be mainly localized to the upper part of the adductor tubercle. Likewise, the SLGA and IMGA were mainly localized at the distal and proximal parts of the epicondyle-shaft transition, respectively. Our results support the feasibility of ultrasound guidance for GA localization in patients with knee osteoarthritis.
Keyword
Figure
-

Fig. 1 Illustration showing the posterior and medial anastomoses that form the arterial network surrounding the knee joint. The small arterial direct termination is from the medial anastomosis to the SMGAd via DGA rather than the SMGA from the posterior anastomosis. Posterior anastomosis: gray colored area with dotted line. Medial anastomosis: red colored area. FA: femoral artery, DGA: descending genicular artery, DO: descending osseous branch, SGTA: superior genicular transverse artery, SMGA: superior medial genicular artery, SMGAs: superficial branch of the SMGA, SMGAd: deep branch of the SMGA, SLGA: superior lateral genicular artery, IMGA: inferior medial genicular artery, ILGA: inferior lateral genicular artery.

Fig. 2 Simplified drawing showing the medial aspect of the knee and the application of the X–Y axis structure for GA localization. As the small arterial direct termination is mainly from the medial anastomosis to SMGA via DGA, the X–Y axis structure was applied at the adductor tubercle, where the trajectory of the SMGA from the posterior anastomosis is from back to front. GA: genicular artery, PA: popliteal artery, SMGA: superior medial genicular artery, IMGA: inferior medial genicular artery.

Fig. 3 Ultrasound-guided images of GAs. Color enhanced shadows (indicated by the white arrow) represent the GAs. (A) Transverse image of SMGA. (B) Longitudinal image of SMGA. (C) Longitudinal image of SLGA. (D) Longitudinal image of IMGA. GA: genicular artery, SMGA: superior medial genicular artery, SLGA: superior lateral genicular artery, IMGA: inferior medial genicular artery.

Fig. 4 Illustration showing placement of the ultrasound generator. An ultrasound generator was aligned with the X axis for transverse view and with the Y axis for longitudinal view. PA: popliteal artery. SMGA: superior medial genicular artery.
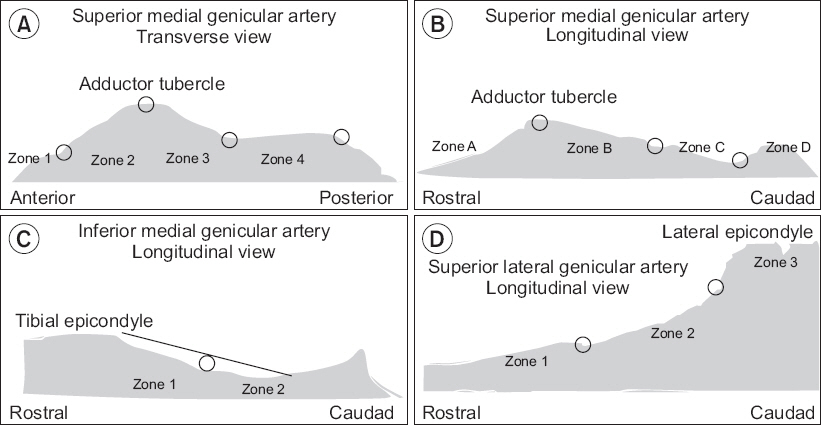
Fig. 5 Clinical research form used for documentation of (A, B) SMGA, (C) IMGA, and (D) SLGA localization. The black line in (C) is representative of the initial fibers of the medial collateral ligament inserting on the tibia. SMGA: superior medial genicular artery. IMGA: inferior medial genicular artery. SLGA: superior lateral genicular artery.
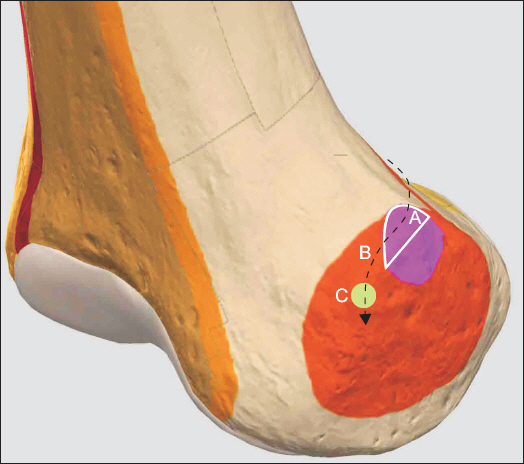
Fig. 6 Hypothetical trajectory of the SMGA and accompanying nerve at the medial aspect of the right femoral epicondyle. 3D-drawing representative of ultrasound-guided SMGA localization. This study found that 91.7% of the SMGA was localized to the upper part of the adductor tubercle. It is hypothesized that the SMGA passes around the upper part of the adductor tubercle before descending to the target point for the SMGN (C: green colored circle) located 1 cm anterior to the peak of the adductor tubercle, as described by Yasar et al. [9]. A: white solid line encircled area, white solid line shows the boundary of the area corresponding to the upper part of the adductor tubercle. B: black dotted line, course of the SMGA. Pink colored area: adductor tubercle, right. Orange colored area: epicondyle, medial femoral, right. SMGA: superior medial genicular artery. SMGN: superior medial genicular nerve.

Fig. 7 Dot plot of the distance from the GAs to the corresponding bony cortex. dSMGAt: distance from the bony cortex to SMGA in the transverse plane. dSMGAl: distance from the bony cortex to SMGA in the longitudinal plane. dIMGAl: distance from the bony cortex to IMGA in the longitudinal plane. dSLGAl: distance from the bony cortex to SLGA in the longitudinal plane. SMGA: superior medial genicular artery. IMGA: inferior medial genicular artery. SLGA: superior lateral genicular artery.

Fig. 8 Scatter plot showing the relationship between dSMGAt and dSMGAl. Blue straight line: fitted values, shaded area: 95% confidence interval. dSMGAt: distance from the bony cortex to SMGA in the transverse plan. dSMGAl: distance from the bony cortex to SMGA in the longitudinal plane. SMGA: superior medial genicular artery.
Reference
-
1. Horner G, Dellon AL. Innervation of the human knee joint and implications for surgery. Clin Orthop Relat Res. 1994; 301:221–6.2. Choi WJ, Hwang SJ, Song JG, Leem JG, Kang YU, Park PH, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011; 152:481–7. DOI: 10.1016/j.pain.2010.09.029. PMID: 21055873.3. Ikeuchi M, Ushida T, Izumi M, Tani T. Percutaneous radiofrequency treatment for refractory anteromedial pain of osteoarthritic knees. Pain Med. 2011; 12:546–51. DOI: 10.1111/j.1526-4637.2011.01086.x. PMID: 21463469.4. Bellini M, Barbieri M. Cooled radiofrequency system relieves chronic knee osteoarthritis pain: the first case-series. Anaesthesiol Intensive Ther. 2015; 47:30–3. DOI: 10.5603/AIT.2015.0003. PMID: 25751290.5. Shen WS, Xu XQ, Zhai NN, Zhou ZS, Shao J, Yu YH. Radiofrequency thermocoagulation in relieving refractory pain of knee osteoarthritis. Am J Ther. 2017; 24:e693–700. DOI: 10.1097/MJT.0000000000000393. PMID: 26938761.6. Protzman NM, Gyi J, Malhotra AD, Kooch JE. Examining the feasibility of radiofrequency treatment for chronic knee pain after total knee arthroplasty. PM R. 2014; 6:373–6. DOI: 10.1016/j.pmrj.2013.10.003. PMID: 24373908.7. Meng M, Waldman RA, Waldman CW, Waldman SD. Ultrasound guided genicular nerve block-a motor sparing technique for the treatment of acute and chronic knee pain. Int J Anesthesiol Res. 2015; 3:37–43.8. Kesikburun S, Yaşar E, Uran A, Adigüzel E, Yilmaz B. Ultrasound-guided genicular nerve pulsed radiofrequency treatment for painful knee osteoarthritis: a preliminary report. Pain Physician. 2016; 19:E751–9. PMID: 27389118.9. Yasar E, Kesikburun S, Kılıç C, Güzelküçük Ü, Yazar F, Tan AK. Accuracy of ultrasound-guided genicular nerve block: a cadaveric study. Pain Physician. 2015; 18:E899–904. PMID: 26431143.10. Kalsi PS, Carrington RJ, Skinner JS. Therapeutic embolization for the treatment of recurrent hemarthrosis after total knee arthroplasty due to an arteriovenous fistula. J Arthroplasty. 2007; 22:1223–5. DOI: 10.1016/j.arth.2006.11.012. PMID: 18078896.11. Kayler DE, Lyttle D. Surgical interruption of patellar blood supply by total knee arthroplasty. Clin Orthop Relat Res 1988. 229:221–7. PMID: 3349681 .12. Kirschner S, Konrad T, Weil EJ, Bühler M. [False aneurysm of the lateral superior genicular artery. A complication after the implantation of a knee prosthesis]. Orthopade. 2004; 33:841–5. German. DOI: 10.1007/s00132-004-0638-z. PMID: 15095036.13. Lazaro LE, Cross MB, Lorich DG. Vascular anatomy of the patella: implications for total knee arthroplasty surgical approaches. Knee. 2014; 21:655–60. DOI: 10.1016/j.knee.2014.03.005. PMID: 24767718.14. Sung-Yoon W, Lee YI, Hun-Mu Y. Anatomy of superior medial genicular artery: a short cadaveric report. Clin Anat. 2016; 29:798–9. DOI: 10.1002/ca.22707. PMID: 26940044.15. Franco CD, Buvanendran A, Petersohn JD, Menzies RD, Menzies LP. Innervation of the anterior capsule of the human knee: implications for radiofrequency ablation. Reg Anesth Pain Med. 2015; 40:363–8. DOI: 10.1097/AAP.0000000000000269. PMID: 26066383.16. Shahid S, Saghir N, Cawley O, Saujani S. A cadaveric study of the branching pattern and diameter of the genicular arteries: a focus on the middle genicular artery. J Knee Surg. 2015; 28:417–24. DOI: 10.1055/s-0035-1549021. PMID: 25892007.17. Huang D, Wang HW, Xu DC, Wang HG, Wu WZ, Zhang HR. An anatomic and clinical study of the adductor magnus tendon-descending genicular artery bone flap. Clin Anat. 2011; 24:77–83. DOI: 10.1002/ca.21060. PMID: 20890971.18. Scheibel MT, Schmidt W, Thomas M, von Salis-Soglio G. A detailed anatomical description of the subvastus region and its clinical relevance for the subvastus approach in total knee arthroplasty. Surg Radiol Anat. 2002; 24:6–12. DOI: 10.1007/s00276-002-0004-y. PMID: 12197013.19. Sabalbal M, Johnson M, McAlister V. Absence of the genicular arterial anastomosis as generally depicted in textbooks. Ann R Coll Surg Engl. 2013; 95:405–9. DOI: 10.1308/003588413X13629960046831. PMID: 24025288. PMCID: PMC4188287.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the efficacy of genicular nerve phenol neurolysis and radiofrequency ablation for pain management in patients with knee osteoarthritis
- Pseudoaneurysm of the Medial Superior Genicular Artery after Arthroscopic Partial Meniscectomy
- Comparison of ultrasound guided pulsed radiofrequency of genicular nerve with local anesthetic and steroid block for management of osteoarthritis knee pain
- Usefulness of Ultrasound-guided Mammotome Biopsy for Microcalcification
- Investigation of the existence of and a block technique for the inferior lateral genicular nerve: cadaveric study
