Sequential CT Findings in Two Cases of Immunoglobulin G4-Related Lung Disease: Focused on Disease Progression
- Affiliations
-
- 1Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 2Department of Radiology, Kangbuk Samsung Hospital, Seoul, Korea. syohammd@hanmail.net
- KMID: 2422905
- DOI: http://doi.org/10.3348/jksr.2018.79.5.276
Abstract
- Immunoglobulin G4 (IgG4)-related lung disease has been actively studied over the past few years. Radiologic findings of IgG4-related lung disease vary among patients, but there are no long-term follow up studies regarding variations in imaging features over the course of disease progression. In two cases with relatively long-term follow up, diverse early and late computed tomography (CT) findings of IgG4-related lung disease are reviewed in this report. In contrast to nodular or diffuse ground-glass opacity, which was predominantly noted in CT scans at earlier stages of disease, honeycombing and traction bronchiectasis were regarded as late radiologic manifestations. Solid nodules might be visible in both early and late stages; however, development of new solid nodules and enlargement of preexisting nodules could occur during disease progression. Interlobular septal thickening and mediastinal/hilar lymphadenopathy were persistent, even in later stages of the disease. These findings might be useful in making an accurate and timely diagnosis of IgG4-related lung disease.
MeSH Terms
Figure
-

Fig. 1 Contrast enhanced serial chest CT scans in a 73-year-old male (case 1) with immunoglobulin G4-related lung disease. A. Spiculated nodular consolidation with air bronchogram is shown in the right upper lobe. B. After 17 months, follow-up chest CT scan reveals a mass larger than 5 cm in the right upper lobe. C. Interlobular septal thickening with satellite nodules are shown in both upper lobes (left), and diffuse and nodular wall thickening of the trachea and esophagus with interval aggravation is simultaneously noted in this CT scan (right).
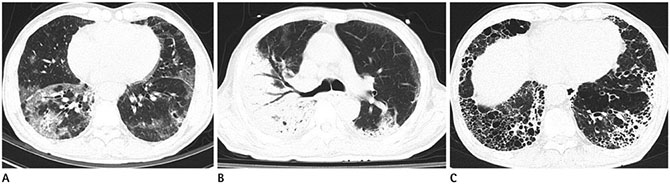
Fig. 2 Serial chest CT scans in a 65-year-old male (case 2) with immunoglobulin G4-related lung disease. A. Multifocal diffuse and patchy ground-glass opacities are noted in the bilateral lungs. B. In the follow-up CT taken 1 month later, extensive consolidations with air bronchogram are shown in both lungs with right lung predominancy. C. The last follow-up CT scan taken in 40 months reveals honeycombing and traction bronchiectasis in both basal lungs.
Reference
-
1. Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22:21–30.
Article2. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001; 344:732–738.
Article3. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.
Article4. Matsui S, Hebisawa A, Sakai F, Yamamoto H, Terasaki Y, Kurihara Y, et al. Immunoglobulin G4-related lung disease: clinicoradiological and pathological features. Respirology. 2013; 18:480–487.
Article5. Ryu JH, Sekiguchi H, Yi ES. Pulmonary manifestations of immunoglobulin G4-related sclerosing disease. Eur Respir J. 2012; 39:180–186.
Article6. Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Kobayashi T, et al. Immunoglobulin G4–related lung disease: CT findings with pathologic correlations. Radiology. 2009; 251:260–270.
Article7. Yamamoto M, Takahashi H, Ishigami K, Yajima H, Shimizu Y, Tabeya T, et al. Relapse patterns in IgG4-related disease. Ann Rheum Dis. 2012; 71:1755.8. Shimizu Y, Yamamoto M, Naishiro Y, Sudoh G, Ishigami K, Yajima H, et al. Necessity of early intervention for IgG4-related disease--delayed treatment induces fibrosis progression. Rheumatology (Oxford). 2013; 52:679–683.
Article9. Kobayashi H, Shimokawaji T, Kanoh S, Motoyoshi K, Aida S. IgG4-positive pulmonary disease. J Thorac Imaging. 2007; 22:360–362.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunoglobulin G4-Related Lung Disease Mimicking Lung Cancer: Two Case Reports
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Immunoglobulin G4-Related Lung Disease with Waxing and Waning Pulmonary Infiltrates: A Case Report
- Unusual Manifestation of Immunoglobulin G4-Related Disease Involving the Retroperitoneum: A Case Report
- Immunoglobulin G4-related sclerosing cholangitis
