Endoscopic Features of Mucous Cap Polyps: A Way to Predict Serrated Polyps
- Affiliations
-
- 1Division of Gastroenterology and Hepatology, UConn Health, Farmington, CT, USA. moy@uchc.edu
- 2Department of Pathology, UConn Health, Farmington, CT, USA.
- 3Connecticut Institute for Clinical & Translational Science, UConn Health, Farmington, CT, USA.
- KMID: 2419709
- DOI: http://doi.org/10.5946/ce.2017.155
Abstract
- BACKGROUND/AIMS
The aims of the study were to identify whether a mucous-cap predicts the presence of serrated polyps, and to determine whether additional endoscopic findings predict the presence of a sessile serrated adenomas/polyp (SSA/P).
METHODS
We analyzed 147 mucous-capped polyps with corresponding histology, during 2011-2014. Eight endoscopic features (presence of borders, elevation, rim of debris, location in the colon, size ≥10 mm, varicose vessels, nodularity, and alteration in mucosal folds) of mucous-capped polyps were examined to see if they can predict SSA/Ps.
RESULTS
A total of 86% (n=126) of mucous-capped polyps were from the right sided serrated pathway (right-sided hyperplastic [n=83], SSA/Ps [n=43], traditional serrated adenoma [n=1]), 10% (n=15) were left-sided hyperplastic polyps, and 3% (n=5) were from the adenoma-carcinoma sequence. The presence of a mucous cap combined with varicose vessels was the only significant predictor for SSA/Ps. The other seven characteristics were not found to be statistically significant for SSA/Ps, although location in the colon and the presence of nodularity trended towards significance.
CONCLUSIONS
Our study suggests that mucous-capped polyps have high predictability for being a part of the serrated pathway. Gastroenterologists should be alert for a mucous-capped polyp with varicose veins, as these lesions have a higher risk of SSA/P.
Figure
-

Fig. 1. (A) An 8 mm mucous-capped polyp in the ascending colon with a distinct border, elevation, and rim of debris. The polyp is ≤10 mm, without varicose vessels, nodular surface, and altering contour folds. The histology is a hyperplastic polyp. (B) A 15 mm mucous-capped polyp in the ascending colon with size ≥10 mm, a distinct border, elevation, rim of debris, and altering contour folds. The polyp is without varicose vessels and a nodular surface. The histology is a hyperplastic polyp. (C) The histology on hematoxylin and eosin (H&E) stain is a hyperplastic polyp. The crypts are elongated but straight, narrow, and hyperchromatic with an ordinary base (×40). (D) The histology on H&E stain is a hyperplastic polyp (×100).

Fig. 2. (A) A 25 mm mucous-capped polyp in the ascending colon with size ≥10 mm, a distinct border, varicose vessels, and nodular surface. The polyp is without elevation, altering contour fold, and rim of debris. The histology is an sessile serrated adenomas/polyp (SSA/P). (B) The histology on hematoxylin and eosin (H&E) stain is an SSA/P. Disorganized, markedly dilated crypts showing extension of goblet cells to the base, and sideways growth of the crypt base is shown (×40). (C) A 6 mm mucous-capped polyp in the ascending colon with distinct borders, rim of debris, and varicose vessels. The size of the polyp is ≤10 mm, without a nodular surface, and altering contour fold. The histology is an SSA/P. (D) The histology on H&E stain is an SSA/P. Disorganized, markedly dilated crypts showing extension of goblet cells to the base, and sideways growth of the crypt base is shown (×100).

Fig. 3. (A) A 15 mm mucous-capped polyp in ascending colon with size ≥10 mm, distinct border, elevation, varicose vessels, and nodular surface. The polyp is without a rim of debris and doesn’t alter contour folds. The histology is a traditional serrated adenoma (TSA). (B) Features of a TSA on hematoxylin and eosin stain show low grade dysplasia with serration separating it from an ordinary tubular adenoma. Note the presence of an eosinophilic cytoplasm of the surface epithelial columnar cells (×200).
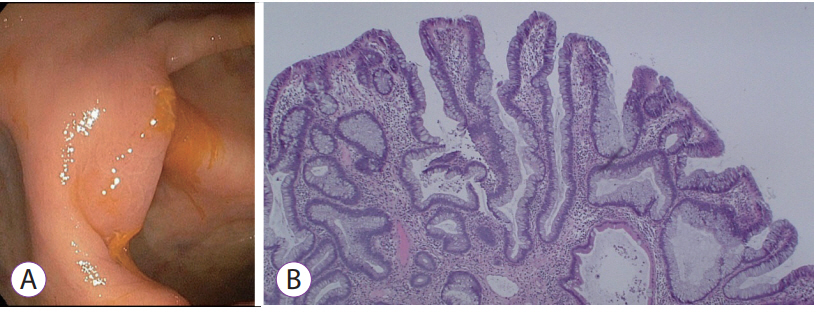
Fig. 4. (A) A 12 mm mucous-capped polyp in cecum with size ≥10 mm, distinct border, elevation, varicose vessels, nodular surface, and altering contour folds. The polyp is without a rim of debris. The histology is a tubular adenoma. (B) Tubular Adenoma is shown on hematoxylin and eosin stain (×100).
Cited by 1 articles
-
How to Detect Sessile Serrated Adenoma/Polyps
Eun Ran Kim, Dong Kyung Chang
Clin Endosc. 2018;51(4):313-314. doi: 10.5946/ce.2018.108.
Reference
-
1. Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988; 319:525–532.
Article2. Sillars-Hardebol AH, Carvalho B, van Engeland M, Fijneman RJ, Meijer GA. The adenoma hunt in colorectal cancer screening: defining the target. J Pathol. 2012; 226:1–6.
Article3. East JE, Saunders BP, Jass JR. Sporadic and syndromic hyperplastic polyps and serrated adenomas of the colon: classification, molecular genetics, natural history, and clinical management. Gastroenterol Clin North Am. 2008; 37:25–46, v.
Article4. Arnold CA, Montgomery E, Iacobuzio-Donahue CA. The serrated pathway of neoplasia: new insights into an evolving concept. Diagn Histopathol (Oxf). 2011; 17:367–375.
Article5. Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology. 2010; 138:2088–2100.
Article6. Torlakovic E, Skovlund E, Snover DC, Torlakovic G, Nesland JM. Morphologic reappraisal of serrated colorectal polyps. Am J Surg Pathol. 2003; 27:65–81.
Article7. Tadepalli US, Feihel D, Miller KM, et al. A morphologic analysis of sessile serrated polyps observed during routine colonoscopy (with video). Gastrointest Endosc. 2011; 74:1360–1368.
Article8. Bressler B, Paszat LF, Chen Z, Rothwell DM, Vinden C, Rabeneck L. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology. 2007; 132:96–102.
Article9. Baxter NN, Goldwasser MA, Paszat LF, Saskin R, Urbach DR, Rabeneck L. Association of colonoscopy and death from colorectal cancer. Ann Intern Med. 2009; 150:1–8.
Article10. Hetzel JT, Huang CS, Coukos JA, et al. Variation in the detection of serrated polyps in an average risk colorectal cancer screening cohort. Am J Gastroenterol. 2010; 105:2656–2664.
Article11. de Wijkerslooth TR, Stoop EM, Bossuyt PM, et al. Differences in proximal serrated polyp detection among endoscopists are associated with variability in withdrawal time. Gastrointest Endosc. 2013; 77:617–623.
Article12. Kahi CJ, Hewett DG, Norton DL, Eckert GJ, Rex DK. Prevalence and variable detection of proximal colon serrated polyps during screening colonoscopy. Clin Gastroenterol Hepatol. 2011; 9:42–46.
Article13. Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013; 144:74–80.e1.
Article14. Murakami T, Sakamoto N, Ritsuno H, et al. Distinct endoscopic characteristics of sessile serrated adenoma/polyp with and without dysplasia/carcinoma. Gastrointest Endosc. 2017; 85:590–600.
Article15. Parente F, Marino B, Crosta C. Bowel preparation before colonoscopy in the era of mass screening for colo-rectal cancer: a practical approach. Dig Liver Dis. 2009; 41:87–95.
Article16. Chiu HM, Lin JT, Lee YC, et al. Different bowel preparation schedule leads to different diagnostic yield of proximal and nonpolypoid colorectal neoplasm at screening colonoscopy in average-risk population. Dis Colon Rectum. 2011; 54:1570–1577.
Article17. Harewood GC, Sharma VK, de Garmo P. Impact of colonoscopy preparation quality on detection of suspected colonic neoplasia. Gastrointest Endosc. 2003; 58:76–79.
Article18. Pereyra L, Gómez EJ, González R, et al. Finding sessile serrated adenomas: is it possible to identify them during conventional colonoscopy? Dig Dis Sci. 2014; 59:3021–3026.
Article19. Rustagi T, Rangasamy P, Myers M, et al. Sessile serrated adenomas in the proximal colon are likely to be flat, large and occur in smokers. World J Gastroenterol. 2013; 19:5271–5277.
Article20. Bauer VP, Papaconstantinou HT. Management of serrated adenomas and hyperplastic polyps. Clin Colon Rectal Surg. 2008; 21:273–279.
Article21. Zhu H, Zhang G, Yi X, et al. Histology subtypes and polyp size are associated with synchronous colorectal carcinoma of colorectal serrated polyps: a study of 499 serrated polyps. Am J Cancer Res. 2015; 5:363–374.22. Rex DK, Ahnen DJ, Baron JA, et al. Serrated lesions of the colorectum: review and recommendations from an expert panel. Am J Gastroenterol. 2012; 107:1315–1329. quiz 1314, 1330.
Article23. Saito S, Tajiri H, Ikegami M. Serrated polyps of the colon and rectum: endoscopic features including image enhanced endoscopy. World J Gastrointest Endosc. 2015; 7:860–871.
Article24. Mäkinen MJ. Colorectal serrated adenocarcinoma. Histopathology. 2007; 50:131–150.
Article25. Carr NJ, Mahajan H, Tan KL, Hawkins NJ, Ward RL. Serrated and non-serrated polyps of the colorectum: their prevalence in an unselected case series and correlation of BRAF mutation analysis with the diagnosis of sessile serrated adenoma. J Clin Pathol. 2009; 62:516–518.
Article26. Kim KM, Lee EJ, Ha S, et al. Molecular features of colorectal hyperplastic polyps and sessile serrated adenoma/polyps from Korea. Am J Surg Pathol. 2011; 35:1274–1286.
Article27. Spring KJ, Zhao ZZ, Karamatic R, et al. High prevalence of sessile serrated adenomas with BRAF mutations: a prospective study of patients undergoing colonoscopy. Gastroenterology. 2006; 131:1400–1407.
Article28. Gurudu SR, Heigh RI, De Petris G, et al. Sessile serrated adenomas: demographic, endoscopic and pathological characteristics. World J Gastroenterol. 2010; 16:3402–3405.
Article29. Hazewinkel Y, López-Cerón M, East JE, et al. Endoscopic features of sessile serrated adenomas: validation by international experts using high-resolution white-light endoscopy and narrow-band imaging. Gastrointest Endosc. 2013; 77:916–924.
Article30. Nakao Y, Saito S, Ohya T, et al. Endoscopic features of colorectal serrated lesions using image-enhanced endoscopy with pathological analysis. Eur J Gastroenterol Hepatol. 2013; 25:981–988.
Article31. Uraoka T, Higashi R, Horii J, et al. Prospective evaluation of endoscopic criteria characteristic of sessile serrated adenomas/polyps. J Gastroenterol. 2015; 50:555–563.
Article32. East JE, Suzuki N, Bassett P, et al. Narrow band imaging with magnification for the characterization of small and diminutive colonic polyps: pit pattern and vascular pattern intensity. Endoscopy. 2008; 40:811–817.
Article33. Yamashina T, Takeuchi Y, Uedo N, et al. Diagnostic features of sessile serrated adenoma/polyps on magnifying narrow band imaging: a prospective study of diagnostic accuracy. J Gastroenterol Hepatol. 2015; 30:117–123.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Diagnosis, Treatment, and Follow-up of Serrated Polyps
- Sessile Serrated Adenoma with High-grade Dysplasia
- External Validation of the Endoscopic Features of Sessile Serrated Adenomas in Expert and Trainee Colonoscopists
- Serrated Adenoma with Adenocarcinoma of Stomach Treated by Endoscopic Submucosal Dissection
- Optical diagnosis by near-focus versus normal-focus narrow band imaging colonoscopy in colorectal polyps based on combined NICE and WASP classification: a randomized controlled trial
