Carotid Intraplaque Hemorrhage Imaging: Diagnostic Value of High Signal Intensity Time-of-Flight MR Angiography Compared with Magnetization-Prepared Rapid Acquisition with Gradient-Echo Sequencing
- Affiliations
-
- 1Student of Medical School, Chonbuk National University, Jeollabuk-do, Korea.
- 2Radiology and Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeollabuk-do, Korea. kwak8140@jbnu.ac.kr
- KMID: 2415887
- DOI: http://doi.org/10.13104/imri.2018.22.2.94
Abstract
- PURPOSE
To determine the value of the appearance of the high signal intensity halo sign for detecting carotid intraplaque hemorrhage (IPH) on maximum intensity projection (MIP) of time-of-flight (TOF) MR angiography (MRA), based on high signal intensity on magnetization-prepared rapid acquisition with gradient-echo (MPRAGE) sequencing.
MATERIALS AND METHODS
A total of 78 carotid arteries in 65 patients with magnetization-prepared rapid acquisition gradient-echo (MPRAGE) positive on carotid plaque MR imaging were included in this study. High-resolution MR imaging was performed on a 3.0-T scanner prior to carotid endarterectomy or carotid artery stenting. Fast spin-echo T1- and T2-weighted axial imaging, TOF, and MPRAGE sequences were obtained. Carotid plaques with high signal intensity on MPRAGE > 200% that of adjacent muscle on at least two consecutive slices were defined as showing IPH. Halo sign of high signal intensity around the carotid artery was found on MIP from TOF MRA. Continuous and categorical variables were compared among groups using the Mann-Whitney test and Fisher's exact tests.
RESULTS
Of these 78 carotid arteries, 53 appeared as a halo sign on the TOF MRA. The total IPH volume of patients with a positive halo sign was significantly higher than that of patients without a halo sign (75.0 ± 86.8 vs. 16.3 ± 18.2, P = 0.001). The maximum IPH axial wall area in patients with a positive halo sign was significantly higher than that of patients without a halo sign (11.3 ± 9.9 vs. 3.7 ± 3.6, P = 0.000).
CONCLUSION
High signal intensity halo of IPH on MIP of TOF MRA is associated with total volume and maximal axial wall area of IPH.
MeSH Terms
Figure
-
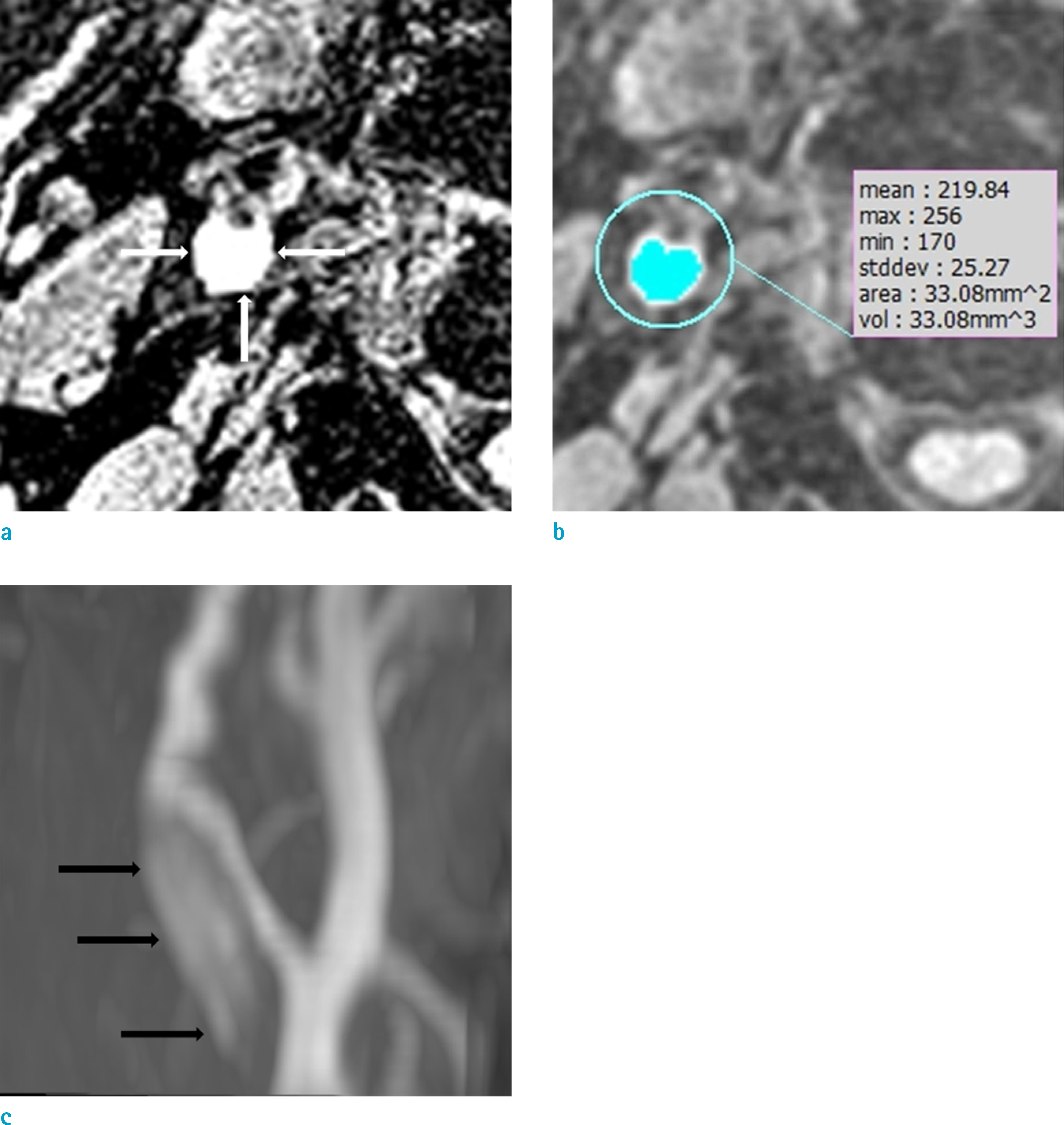
Fig. 1. Intraplaque hemorrhage and measurement of intraplaque hemorrhage volume. (a) Intraplaque hemorrhage of high signal intensity on MPRAGE (magnetization-prepared rapid acquisition gradient-echo) sequence (arrows). (b) Semiautomatic measurement of intraplaque hemorrhage volume of the area of signal intensity of > 200% of signal intensity of the adjacent muscle. (c) Intraplaque hemorrhage-positive on maximum intensity projection images of time-of-flight MR angiography shows a hyperintense region in the vessel wall without connection to the lumen (arrows).
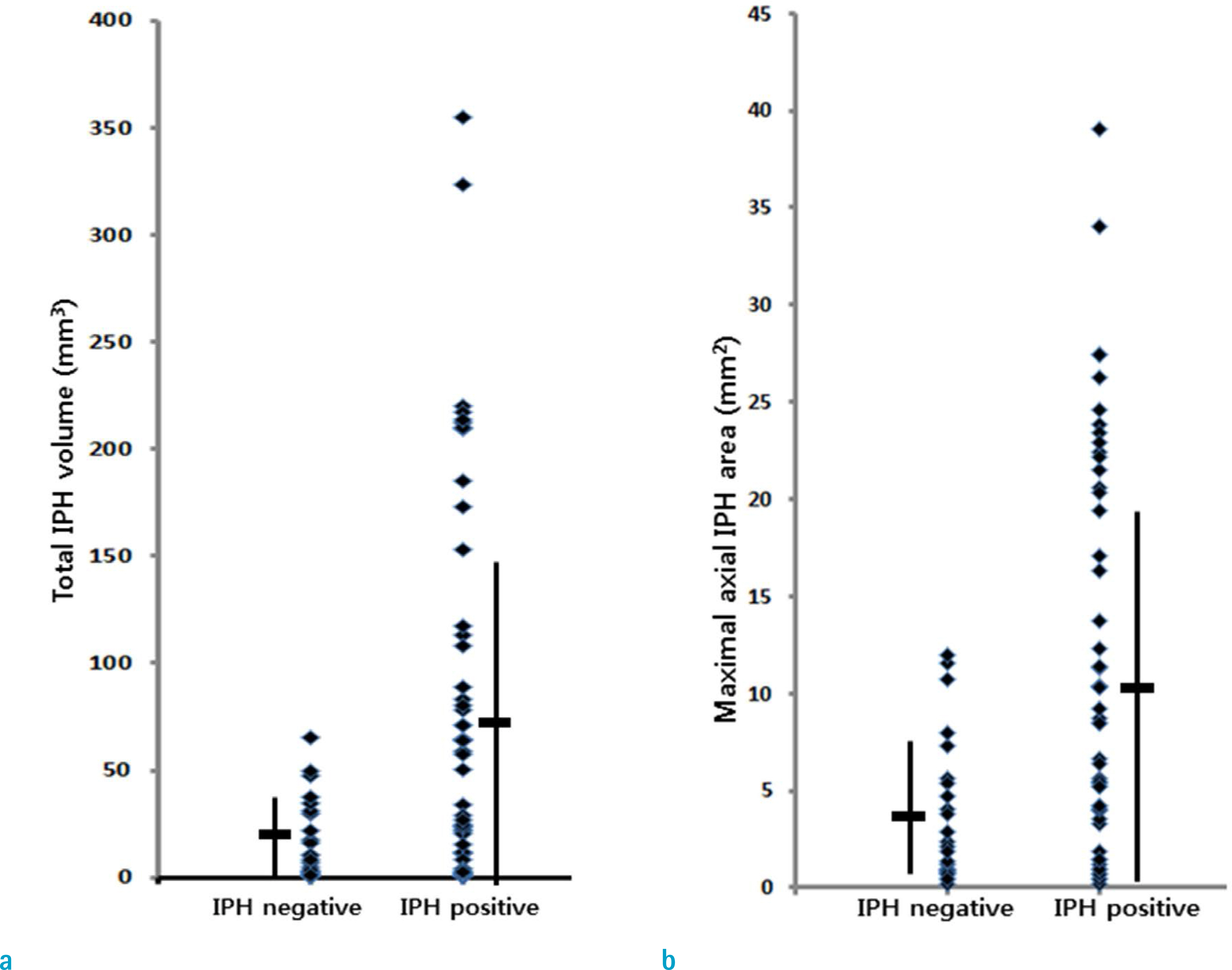
Fig. 2. Intraplaque hemorrhage (IPH) volume and maximal axial wall area of IPH between positive halo sign and negative halo sign on maximum intensity projection (MIP) images of time-of-flight MR angiography. (a) Total IPH volume is significantly larger in the positive halo sign group than in the negative halo sign group on MIP images. (b) The maximal axial wall area of IPH is also significantly larger in the positive halo sign group than in the negative halo sign group on MIP images.
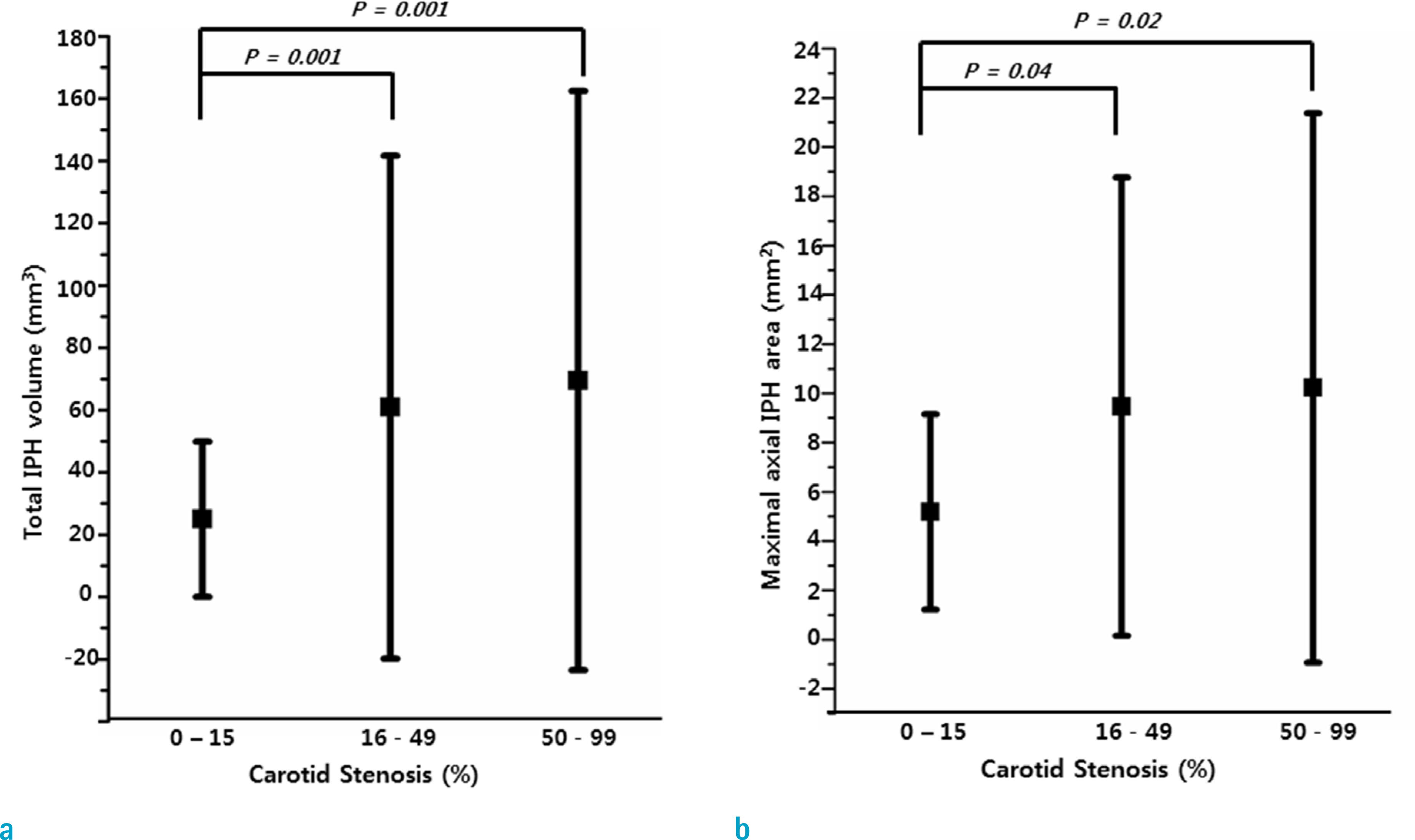
Fig. 3. Intraplaque hemorrhage (IPH) volume and maximal axial wall area of IPH as carotid stenosis categories. (a) Total volume of IPH of carotid arteries with 16–50% and 51–99% was significantly larger than that of carotid arteries with 0–15%. (b) Maximal axial wall area of IPH of carotid arteries with 16–50% and 51–99% was significantly larger than that of carotid arteries with 0–15%.
Reference
-
References
1. Yamada K, Song Y, Hippe DS, et al. Quantitative evaluation of high intensity signal on MIP images of carotid atherosclerotic plaques from routine TOF-MRA reveals elevated volumes of intraplaque hemorrhage and lipid rich necrotic core. J Cardiovasc Magn Reson. 2012; 14:81.
Article2. Sun J, Underhill HR, Hippe DS, Xue Y, Yuan C, Hatsukami TS. Sustained acceleration in carotid atherosclerotic plaque progression with intraplaque hemorrhage: a longterm time course study. JACC Cardiovasc Imaging. 2012; 5:798–804.3. Saam T, Hetterich H, Hoffmann V, et al. Meta-analysis and systematic review of the predictive value of carotid plaque hemorrhage on cerebrovascular events by magnetic resonance imaging. J Am Coll Cardiol. 2013; 62:1081–1091.
Article4. Hosseini AA, Simpson RJ, Altaf N, Bath PM, MacSweeney ST, Auer DP. Magnetic resonance imaging plaque hemorrhage for risk stratification in carotid artery disease with moderate risk under current medical therapy. Stroke. 2017; 48:678–685.
Article5. Yoon W, Kim SK, Park MS, Chae HJ, Kang HK. Safety of protected carotid artery stenting in patients with severe carotid artery stenosis and carotid intraplaque hemorrhage. AJNR Am J Neuroradiol. 2012; 33:1027–1031.
Article6. Yoshimura S, Yamada K, Kawasaki M, et al. High-intensity signal on time-of-flight magnetic resonance angiography indicates carotid plaques at high risk for cerebral embolism during stenting. Stroke. 2011; 42:3132–3137.
Article7. van den Bouwhuijsen QJ, Selwaness M, Tang H, et al. Change in carotid intraplaque hemorrhage in community-dwelling subjects: a follow-up study using serial MR imaging. Radiology. 2017; 282:526–533.
Article8. Ota H, Yarnykh VL, Ferguson MS, et al. Carotid intraplaque hemorrhage imaging at 3.0-T MR imaging: comparison of the diagnostic performance of three T1-weighted sequences. Radiology. 2010; 254:551–563.
Article9. Yim YJ, Choe YH, Ko Y, et al. High signal intensity halo around the carotid artery on maximum intensity projection images of time-of-flight MR angiography: a new sign for intraplaque hemorrhage. J Magn Reson Imaging. 2008; 27:1341–1346.
Article10. Yarnykh VL, Terashima M, Hayes CE, et al. Multicontrast black-blood MRI of carotid arteries: comparison between 1.5 and 3 tesla magnetic field strengths. J Magn Reson Imaging. 2006; 23:691–698.
Article11. Underhill HR, Yarnykh VL, Hatsukami TS, et al. Carotid plaque morphology and composition: initial comparison between 1.5- and 3.0-T magnetic field strengths. Radiology. 2008; 248:550–560.
Article12. Singh N, Moody AR, Gladstone DJ, et al. Moderate carotid artery stenosis: MR imaging-depicted intraplaque hemorrhage predicts risk of cerebrovascular ischemic events in asymptomatic men. Radiology. 2009; 252:502–508.
Article13. Sun J, Balu N, Hippe DS, et al. Subclinical carotid atherosclerosis: short-term natural history of lipid-rich necrotic core–a multicenter study with MR imaging. Radiology. 2013; 268:61–68.
Article14. Mughal MM, Khan MK, DeMarco JK, Majid A, Shamoun F, Abela GS. Symptomatic and asymptomatic carotid artery plaque. Expert Rev Cardiovasc Ther. 2011; 9:1315–1330.
Article15. Gupta A, Baradaran H, Kamel H, et al. Intraplaque high-intensity signal on 3D time-of-flight MR angiography is strongly associated with symptomatic carotid artery stenosis. AJNR Am J Neuroradiol. 2014; 35:557–561.
Article16. Saito A, Sasaki M, Ogasawara K, et al. Carotid plaque signal differences among four kinds of T1-weighted magnetic resonance imaging techniques: a histopathological correlation study. Neuroradiology. 2012; 54:1187–1194.
Article17. Kwak HS, Yang HJ, Hwang SB, Chung GH. Carotid wall imaging with routine brain MRI to facilitate early detection of carotid plaque and intraplaque hemorrhage. J Stroke. 2017; 19:107–108.
Article18. McNally JS, Kim SE, Yoon HC, et al. Carotid magnetization-prepared rapid acquisition with gradient-echo signal is associated with acute territorial cerebral ischemic events detected by diffusion-weighted MRI. Circ Cardiovasc Imaging. 2012; 5:376–382.
Article19. Park JS, Kwak HS, Lee JM, Koh EJ, Chung GH, Hwang SB. Association of carotid intraplaque hemorrhage and territorial acute infarction in patients with acute neurological symptoms using carotid magnetization-prepared rapid acquisition with gradient-echo. J Korean Neurosurg Soc. 2015; 57:94–99.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Association of Carotid Intraplaque Hemorrhage and Territorial Acute Infarction in Patients with Acute Neurological Symptoms Using Carotid Magnetization-Prepared Rapid Acquisition with Gradient-Echo
- Carotid Intraplaque Hemorrhage is Associated with Acute Cerebral Ischemic Events and Progression of Stenosis on Magnetic Resonance Imaging
- Diagnostic Criteria of T1-Weighted Imaging for Detecting Intraplaque Hemorrhage of Vertebrobasilar Artery Based on Simultaneous Non-Contrast Angiography and Intraplaque Hemorrhage Imaging
- Magnetization Transfer Contrast Angiography for Organized Thrombosed Intracranial Aneurysm in TOF MR Angiography: a Case Report
- Symptomatic Isolated Middle Cerebral Artery Dissection: High Resolution MR Findings
