Liver Abscess Secondary to Perforation after Duodenal Endoscopic Resection
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. endoksj@gmail.com
- 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Radiology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2415487
- DOI: http://doi.org/10.4166/kjg.2018.71.5.286
Abstract
- Duodenal perforation is a complication of endoscopic mucosal resection. Liver abscess secondary to iatrogenic perforation is extremely rare. A 43-year-old female visited the hospital to remove a sub-epithelial tumor on the duodenal bulb. After endoscopic mucosal resection with band ligation, duodenal perforation occurred. Endoscopic closure was performed successfully using a clipping device to manage duodenal perforation. After 4 weeks, the patient visited our outpatient clinic due to abdominal pain and fever. Abdominal computed tomography showed liver abscess that involved segment three. Liver abscess was resolved with a 10-week antibiotic treatment. To the best of our knowledge, no case of liver abscess secondary to duodenal perforation by endoscopic resection was reported to date in Korea. Here, we report a case of liver abscess caused by a duodenal perforation after endoscopic mucosal resection.
MeSH Terms
Figure
-
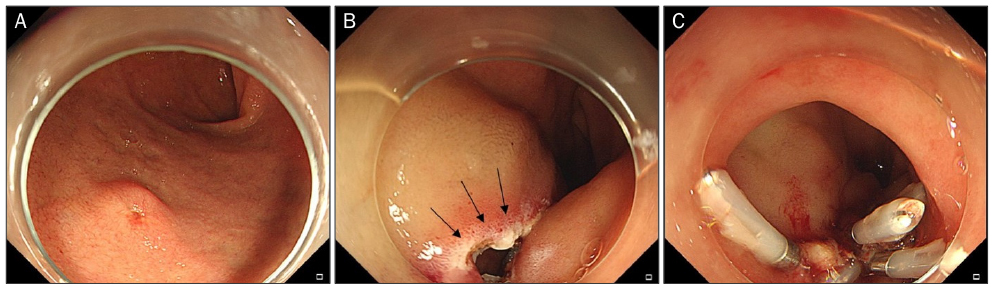
Fig. 1 (A) Yellowish sub-epithelial tumor with a size of about 0.5 cm with biopsy-induced erosion on the top of the lesion on the duodenal bulb. (B) Occurrence of perforation at the lateral resection margin (arrows) after endoscopic mucosal resection with band ligation. (C) Successful closure of perforation with endoscopic clips.
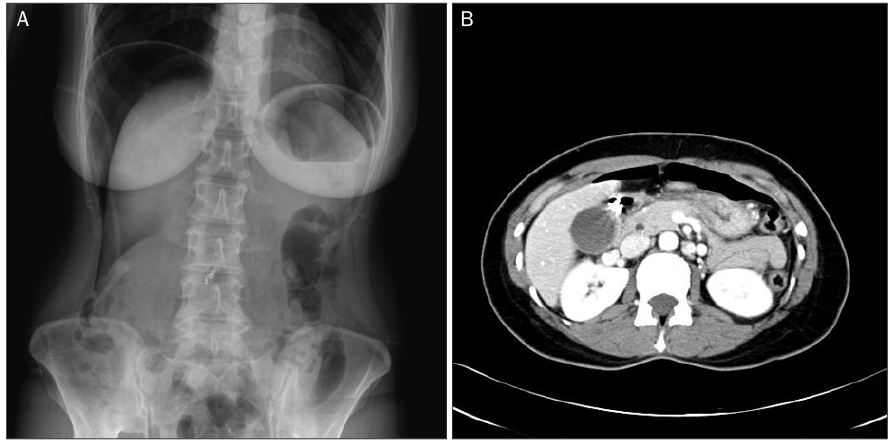
Fig. 2 (A) Abdominal X-ray after endoscopic resection showing bilateral sub-diaphragmatic free air. (B) Abdominal computed tomography scan showing the presence of pneumoperitoneum and clips in the duodenal bulb.
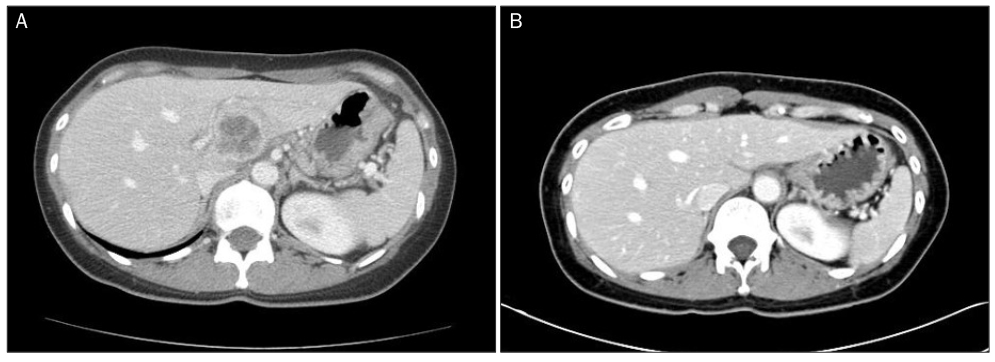
Fig. 3 (A) Liver abscess with a size of 7.5×7.0 cm is observed in the segment three on the abdominal computed tomography. (B) Disappearance of liver abscess on a follow-up study after antibiotic treatment.
Reference
-
1. Huang CJ, Pitt HA, Lipsett PA, et al. Pyogenic hepatic abscess. Changing trends over 42 years. Ann Surg. 1996; 223:600–607.2. Heathfield KWG, Lond MB. Liver abscess following perforated duodenal ulcer. Lancet. 1942; 240:155.
Article3. Kim DH, Lee CH, Jung HK. A case of subcapsular liver abscess secondary to perforating ulcer of gastric cancer. Korean J Gastroenterol. 2010; 56:109–113.
Article4. Chintamani , Singhal V, Lubhana P, Durkhere R, Bhandari S. Liver abscess secondary to a broken needle migration--a case report. BMC Surg. 2003; 3:8.
Article5. Kadowaki Y, Tamura R, Okamoto T, Mori T, Mori T. Ruptured hepatic abscess caused by fish bone penetration of the duodenal wall: report of a case. Surg Today. 2007; 37:1018–1021.
Article6. Jimenez-Fuertes M, Moreno-Posadas A, Ruíz-Tovar J, Durán-Poveda M. Liver abscess secondary to duodenal perforation by fishbone: report of a case. Rev Esp Enferm Dig. 2016; 108:42.7. Allard JC, Kuligowska E. Percutaneous treatment of an intrahepatic abscess caused by a penetrating duodenal ulcer. J Clin Gastroenterol. 1987; 9:603–606.8. Voermans RP, Le Moine O, von Renteln D, et al. Efficacy of endoscopic closure of acute perforations of the gastrointestinal tract. Clin Gastroenterol Hepatol. 2012; 10:603–608.
Article9. Park YM, Cho E, Kang HY, Kim JM. The effectiveness and safety of endoscopic submucosal dissection compared with endoscopic mucosal resection for early gastric cancer: a systematic review and metaanalysis. Surg Endosc. 2011; 25:2666–2677.
Article10. Ohkuwa M, Hosokawa N, Boku N, Ohtu A, Tajiri H, Yoshida S. New endoscopic treatment for intramucosal gastric tumors using an insulated-tip diathermic knife. Endoscopy. 2001; 33:221–226.
Article11. Kaneko T, Akamatsu T, Shimodaira K, et al. Nonsurgical treatment of duodenal perforation by endoscopic repair using a clipping device. Gastrointest Endosc. 1999; 50:410–413.
Article12. Bertel CK, van Heerden JA, Sheedy PF 2nd. Treatment of pyogenic hepatic abscesses. Surgical vs percutaneous drainage. Arch Surg. 1986; 121:554–558.13. Choi CS, Seo GS, Cho EY, et al. Comparison of pyogenic liver abscesses based on the origin of infection. Korean J Med. 2008; 75:60–67.14. Maher JA Jr, Reynolds TB, Yellin AE. Successful medical treatment of pyogenic liver abscess. Gastroenterology. 1979; 77:618–622.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Liver Abscess Associated with Duodenal Perforation by a Toothpick
- Retroperitoneal Duodenal Perforation Following a Endoscopic Sphincterotomy: A case report
- Two Cases of Successful Clipping Closure of Iatrogenic Duodenal Perforation Occurred during Endoscopic Procedure
- Endoscopic Suturing for the Prevention and Treatment of Complications Associated with Endoscopic Mucosal Resection of Large Duodenal Adenomas
- A Case of Recurrent Liver Abscess Due to Choledochoduodenal Fistula
