Temporomandibular joint synovial chondromatosis accompanying temporal bone proliferation: A case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, Dankook University College of Dentistry, Cheonan, Korea. wjhan@dankook.ac.kr
- 2Department of Pathology, Dankook University College of Medicine, Cheonan, Korea.
- KMID: 2413927
- DOI: http://doi.org/10.5624/isd.2018.48.2.147
Abstract
- Synovial chondromatosis is a rare metaplastic disease affecting the joints, including the temporomandibular joint (TMJ). Since its symptoms are similar to those of temporomandibular disorders, a careful differential diagnosis is essential. A 50-year-old male patient was referred with the chief complaint of pain and radiopaque masses around the left TMJ on panoramic radiography. Clinically, pre-auricular swelling and resting pain was found, without limitation of mouth opening. On cone-beam computed tomographic images, multiple calcified nodules adjacent to the TMJ and bone proliferation with sclerosis at the articular fossa and eminence were found. T2-weighted magnetic resonance images showed multiple signal-void nodules with high signal effusion in the superior joint space and thickened cortical bone at the articular fossa and eminence. The calcified nodules were removed by surgical excision, but the hypertrophic articular fossa and eminence remained. A histopathological examination confirmed the diagnosis. The patient was followed up few months later without recurrence.
Keyword
MeSH Terms
Figure
-

Fig. 1 Preoperative panoramic image shows loose bodies of various shapes and sizes around the left mandibular condyle, leading to the suspicion of flat hypertrophy of the articular eminence.
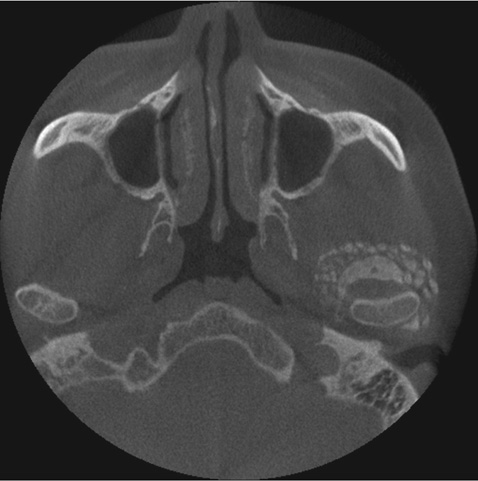
Fig. 2 An axial cone-beam computed tomographic image shows numerous, pebble-like loose bodies surrounding the condyle in all directions except for the medial-posterior side. A large, crescent-shaped, loose body is also seen anterior to the condyle.

Fig. 3 Coronal oblique cone-beam computed tomographic (CBCT) images. A. Loose bodies are seen on the superior and lateral sides of the condyle. Sclerosis and hypertrophy of the glenoid fossa are also seen. B–D. CBCT images anterior to the condyle. B. Loose bodies are seen on the medial and lateral sides. Sclerosis and hypertrophy of the articular eminence are also prominent on the lateral side. C. A large, elliptical loose body among several small loose bodies is seen on the medial and lateral sides. Sclerosis and hypertrophy of the articular eminence are also prominent on both the medial and lateral sides. D. The hypertrophic mass of the articular eminence is seen to be partially detached and sclerosis of the articular eminence is still evident. Small loose bodies are seen inferior to the mass.

Fig. 4 Sagittal cone-beam computed tomographic (CBCT) images. A. A partially detached hypertrophic mass is seen at the anterior slope of the articular eminence. A large loose body is also seen at the posterior side of the condyle, among several small loose bodies. B and C. A large loose body is seen on the anterior side of the condyle. The hypertrophic mass is still seen at the anterior slope of the articular eminence. D. A CBCT image lateral to the condyle shows the partially detached hypertrophic mass at the articular eminence and loose bodies inferior to the mass.

Fig. 5 T1-weighted magnetic resonance images in the closed position. A. A sagittal image at the medial half of the condyle shows loose bodies and the hypertrophic mass as low-signal intensity masses anterior to the condyle and the articular eminence, respectively. B. A coronal image at the anterior side of the condyle shows loose bodies as low-signal intensity masses inferior to the temporal bone and the zygomatic bone, spread across the medial and lateral sides.

Fig. 6 T1-weighted, fat-suppressed magnetic resonance images with contrast enhancement in the closed position. A. A sagittal image at the medial half of the condyle shows the low-signal intensity hypertrophic mass at the anterior slope of the articular eminence, as well as loose bodies surrounded by a high-signal-intensity peripheral wall, corresponding to the synovial membrane. B. A coronal image at the anterior side of the condyle shows low-signal-intensity loose bodies inferior to the temporal bone and the zygomatic bone, surrounded by a high-signal-intensity peripheral wall.

Fig. 7 T2-weighted magnetic resonance images in the closed position. A. A sagittal image at the medial half of the condyle prominently shows a low-signal-intensity hypertrophic mass at the anterior slope of the articular eminence, as well as loose bodies in the high-signal-intensity effusion. B. A coronal image at the anterior side of the condyle shows low-signal-intensity loose bodies inferior to the temporal bone and the zygomatic bone, in the high-signal-intensity effusion.

Fig. 8 A. A low-power view exhibits many small ovoid loose bodies with focal calcification (H&E stain, original magnification ×12.5). B. Higher magnification of the loose body showing vague lobules of hyaline cartilage enclosed by a thin layer of attenuated synovial cells (H&E stain, original magnification ×100).

Fig. 9 Cropped preoperative (A) and postoperative (B) panoramic images in magnified views show the left mandibular condyle region. Through surgical excision, the loose bodies were removed, but the hypertrophic mass of the temporal bone remained.
Reference
-
1. Schulte WC, Rhyne RR. Synovial chondromatosis of temporomandibular joint. Report of a case. Oral Surg Oral Med Oral Pathol. 1969; 28:906–913.2. Tamimi D, Hatcher D. Specialty imaging. Temporomandibular joint. Philadelphia, PA: Elsevier;2016. p. 530–533.3. Testaverde L, Perrone A, Caporali L, Ermini A, Izzo L, D'Angeli I, et al. CT and MR findings in synovial chondromatosis of the temporo-mandibular joint: our experience and review of literature. Eur J Radiol. 2011; 78:414–418.
Article4. Ida M, Yoshitake H, Okoch K, Tetsumura A, Ohbayashi N, Amagasa T, et al. An investigation of magnetic resonance imaging features in 14 patients with synovial chondromatosis of the temporomandibular joint. Dentomaxillofac Radiol. 2008; 37:213–219.
Article5. von Lindern JJ, Theuerkauf I, Niederhagen B, Bergé S, Appel T, Reich RH. Synovial chondromatosis of the temporomandibular joint: clinical, diagnostic, and histomorphologic findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:31–38.
Article6. Matsumoto K, Sato T, Iwanari S, Kameoka S, Oki H, Komiyama K, et al. The use of arthrography in the diagnosis of temporomandibular joint synovial chondromatosis. Dentomaxillofac Radiol. 2013; 42:15388284.
Article7. Liu X, Huang Z, Zhu W, Liang P, Tao Q. Clinical and imaging findings of temporomandibular joint synovial chondromatosis: an analysis of 10 cases and literature review. J Oral Maxillofac Surg. 2016; 74:2159–2168.
Article8. Meng J, Guo C, Yi B, Zhao Y, Luo H, Ma X. Clinical and radiologic findings of synovial chondromatosis affecting the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109:441–448.
Article9. Lim SW, Jeon SJ, Choi SS, Choi KH. Synovial chondromatosis in the temporomandibular joint: a case with typical imaging features and pathological findings. Br J Radiol. 2011; 84:e213–e216.
Article10. Yu Q, Yang J, Wang P, Shi H, Luo J. CT features of synovial chondromatosis in the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97:524–528.
Article11. Wang P, Tian Z, Yang J, Yu Q. Synovial chondromatosis of the temporomandibular joint: MRI findings with pathological comparison. Dentomaxillofac Radiol. 2012; 41:110–116.
Article12. Villacin AB, Brigham LN, Bullough PG. Primary and secondary synovial chondrometaplasia: histopathologic and clinicoradiologic differences. Hum Pathol. 1979; 10:439–451.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary synovial chondromatosis of the temporomandibular joint with temporal involvement
- CASE REPORT OF SYNOVIAL CHONDROMATOSIS IN THE TEMPOROMANDIBULAR JOINT
- Articular loose body, Synovial Chondromatosis of the Temporomandibular Joint: a Case Report
- Temporomandibular joint synovial chondromatosis extending to the temporal bone: a report of two cases
- A clinical Study of Synovial Chondromatosis
