Ann Surg Treat Res.
2018 Jun;94(6):342-345. 10.4174/astr.2018.94.6.342.
Right-sided diaphragmatic rupture in a poly traumatized patient
- Affiliations
-
- 1Department of Trauma Surgery, Chungbuk National University Hospital, Cheongju, Korea. ssulyh@gmail.com
- 2Department of Anesthesiology and Pain Medicine, Chungbuk National University Hospital, Cheongju, Korea.
- 3Department of Trauma Surgery, Cheju Halla General Hospital, Jeju, Korea.
- KMID: 2412405
- DOI: http://doi.org/10.4174/astr.2018.94.6.342
Abstract
- Traumatic diaphragmatic rupture (TDR) is uncommon, and may be associated with other severe life-threatening injuries after blunt trauma. Recently, we experienced a right-sided TDR patient with other multiple life-threatening injuries. A 59-year-old female inflicted with a right-sided TDR accompanied by herniated liver was treated with thoracoscopic exploration. We successfully managed associated life-threatening injuries such as traumatic brain injury and pelvic bone fractures with bleeding, simultaneously.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial chest radiologic findings show elevated right diaphragm (white arrows).
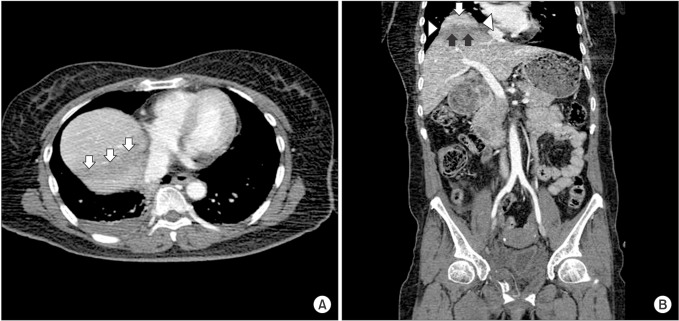
Fig. 2 (A) Abdomen and pelvic CT (APCT) shows an area of hypoattenuation in the dome of the liver (arrows). (B) APCT shows herniation of liver dome through a diaphragmatic rupture (white arrow, hump sign), waistlike constriction of liver (arrowhead, collar sign), and linear area of subtle hypoattenuation (black arrows, band sign).
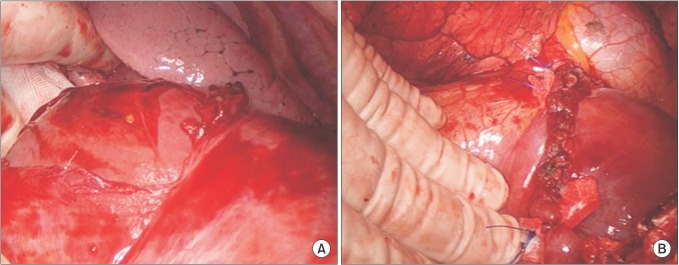
Fig. 3 (A) Operative findings show diaphragmatic rupture with herniation of liver. (B) Operative findings show diaphragmatic repair done by interrupted pledgeted sutures.
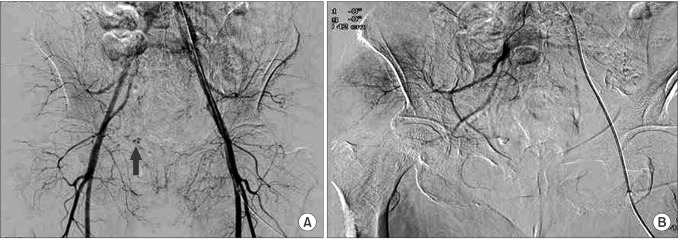
Fig. 4 (A) Pre-embolization angiographic finding showing extravasation (black arrow). (B) Postembolization angiographic finding showing no extravasation.
Reference
-
1. Hanna WC, Ferri LE. Acute traumatic diaphragmatic injury. Thorac Surg Clin. 2009; 19:485–489. PMID: 20112631.
Article2. Scharff JR, Naunheim KS. Traumatic diaphragmatic injuries. Thorac Surg Clin. 2007; 17:81–85. PMID: 17650700.
Article3. Kearney PA, Rouhana SW, Burney RE. Blunt rupture of the diaphragm: mechanism, diagnosis, and treatment. Ann Emerg Med. 1989; 18:1326–1330. PMID: 2589701.
Article4. Thiam O, Konate I, Gueye ML, Toure AO, Seck M, Cisse M, et al. Traumatic diaphragmatic injuries: epidemiological, diagnostic and therapeutic aspects. Springerplus. 2016; 5:1614. PMID: 27652187.
Article5. Vermillion JM, Wilson EB, Smith RW. Traumatic diaphragmatic hernia presenting as a tension fecopneumothorax. Hernia. 2001; 5:158–160. PMID: 11759804.
Article6. Andrus CH, Morton JH. Rupture of the diaphragm after blunt trauma. Am J Surg. 1970; 119:686–693. PMID: 5445992.
Article7. Eren S, Ciris F. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol. 2005; 54:448–459. PMID: 15899350.
Article8. Rodriguez-Morales G, Rodriguez A, Shatney CH. Acute rupture of the diaphragm in blunt trauma: analysis of 60 patients. J Trauma. 1986; 26:438–444. PMID: 3701892.
Article9. Dwivedi S, Banode P, Gharde P, Bhatt M, Ratanlal Johrapurkar S. Treating traumatic injuries of the diaphragm. J Emerg Trauma Shock. 2010; 3:173–176. PMID: 20606795.
Article10. Ties JS, Peschman JR, Moreno A, Mathiason MA, Kallies KJ, Martin RF, et al. Evolution in the management of traumatic diaphragmatic injuries: a multicenter review. J Trauma Acute Care Surg. 2014; 76:1024–1028. PMID: 24662867.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Right Diaphragmatic Rupture Combined with Avulsion of the Right Kidney and Herniation of the Liver into the Thorax
- Delayed presentation of traumatic diaphragmatic rupture with complicated cholecystitis
- Clinical Analysis of Traumatic Diaphragmatic Rupture
- Incidental traumatic right diaphragmatic rupture: a missed case after trauma
- Diagnostic significance of diaphragmatic height index in traumatic diaphragmatic rupture
