Korean J Hepatobiliary Pancreat Surg.
2013 May;17(2):86-88. 10.14701/kjhbps.2013.17.2.86.
Delayed presentation of traumatic diaphragmatic rupture with complicated cholecystitis
- Affiliations
-
- 1Department of Surgery, Kyungpook National University Hospital, Kyungpook National University School of Medicine, Daegu, Korea.
- 2Department of Thoracic and Cardiovascular Surgery, Kyungpook National University Medical Center, Daegu, Korea. bay@knu.ac.kr
- KMID: 1429986
- DOI: http://doi.org/10.14701/kjhbps.2013.17.2.86
Abstract
- The right-sided diaphragmatic rupture is often clinically occulted due to buffering effects of the liver and thus, erroneous diagnosis of such rupture may result in life-threatening conditions. A 44-year-old female who had a history of car accident in 2006 was admitted to our hospital for pleuritic pain. On the chest computed tomography, she was diagnosed with diaphragmatic rupture accompanied by herniation of hypertrophic left liver with complicated cholecystitis and we carried out cholecystectomy, reduction of the liver, pleural drainage, and primary closure of the diaphragm via thoracic approaches. Our case is presented in three unique aspects: herniation of left hemiliver, hypertrophic liver herniated up to the 4th rib level, and combination of complicated cholecystitis. Although the diagnosis of right-sided diaphragmatic rupture can be challenging for the surgeon, an early diagnosis can prevent further complications on the clinical presentation.
MeSH Terms
Figure
-
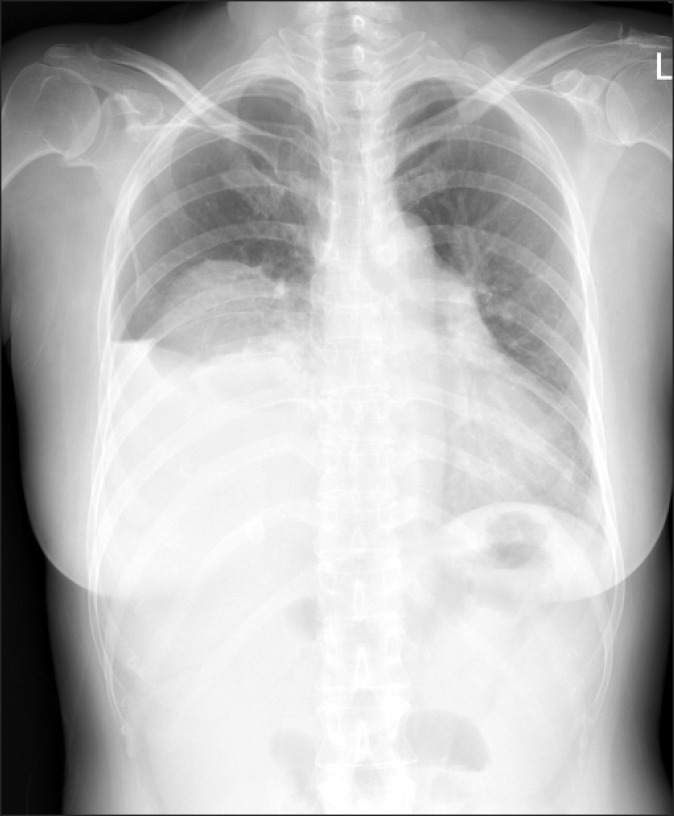
Fig. 1 Chest PA revealing higher positioning of the right hemi-diaphragm.
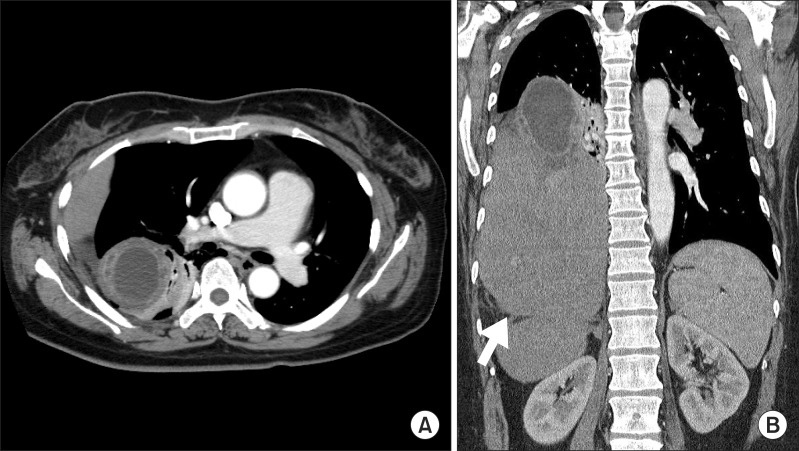
Fig. 2 Chest CT scan showing herniated liver and complicated cholecystitis. (A) Axial view. (B) Coronal view: The arrow demonstrates "the collar sign" of the liver.
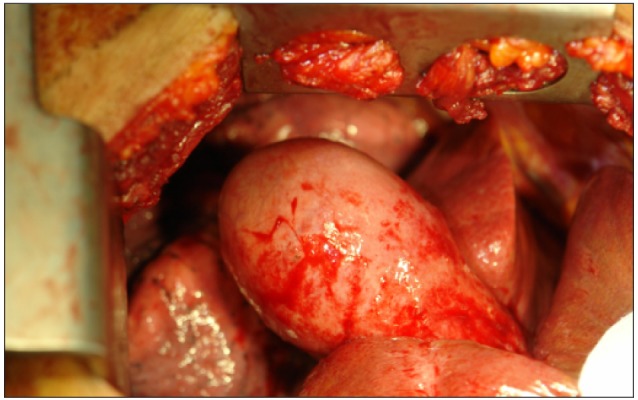
Fig. 3 Intraoperative view of complicated cholecystitis.
Reference
-
1. Wirbel RJ, Mutschler W. Blunt rupture of the right hemi-diaphragm with complete dislocation of the right hepatic lobe: report of a case. Surg Today. 1998; 28:850–852. PMID: 9719010.
Article2. Boulanger BR, Milzman DP, Rosati C, et al. A comparison of right and left blunt traumatic diaphragmatic rupture. J Trauma. 1993; 35:255–260. PMID: 8355305.
Article3. Heiberg E, Wolverson MK, Hurd RN, et al. CT recognition of traumatic rupture of the diaphragm. AJR Am J Roentgenol. 1980; 135:369–372. PMID: 6773345.
Article4. Demos TC, Solomon C, Posniak HV, et al. Computed tomography in traumatic defects of the diaphragm. Clin Imaging. 1989; 13:62–67. PMID: 2743195.
Article5. Holland DG, Quint LE. Traumatic rupture of the diaphragm without visceral herniation: CT diagnosis. AJR Am J Roentgenol. 1991; 157:17–18. PMID: 2048513.
Article6. Gelman R, Mirvis SE, Gens D. Diaphragmatic rupture due to blunt trauma: sensitivity of plain chest radiographs. AJR Am J Roentgenol. 1991; 156:51–57. PMID: 1898570.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Presentarion of Traumatic Diaphragmatic Rupture
- Delayed Presentation of Traumatic Diaphragmatic Hernia
- A Case of Late Presentation of Traumatic Diaphragmatic Hernia in a Child
- Delayed presenting traumatic diaphragmatic hernia: four case reports
- Traumatic Diaphragmatic Hernia with Delayed Presentation in an Adult
