Proper Management of Posttraumatic Tension Pneumocephalus
- Affiliations
-
- 1Department of Neurosurgery, Yeouido St. Mary's Hospital, The Catholic University College of Medicine, Seoul, Korea. plo19@hanmail.net
- KMID: 2394553
- DOI: http://doi.org/10.13004/kjnt.2017.13.2.158
Abstract
- Pneumocephalus is commonly seen after craniofacial injury. The pathogenesis of pneumocephalus has been debated as to whether it was caused by ball valve effect or combined episodic increased pressure within the nasopharynx on coughing. Discontinuous exchange of air and cerebrospinal fluid due to "inverted bottle" effect is assumed to be the cause of it. Delayed tension pneumocephalus is not common, but it requires an active management in order to prevent serious complication. We represent a clinical case of a 57-year-old male patient who fell down from 3 m height, complicated by tension pneumocephalus on 5 months after trauma. We recommend a surgical intervention, but the patient did not want that so we observe the patient. The patient was underwent seizure and meningitis after 7 months after trauma, he came on emergency room on stupor mentality. Tension pneumocephalus may result in a neurologic disturbance due to continued air entrainment and it significantly the likelihood of intracranial infection caused by continued open channel. Tension pneumocephalus threat a life, so need a neurosurgical emergency surgical intervention.
MeSH Terms
Figure
-
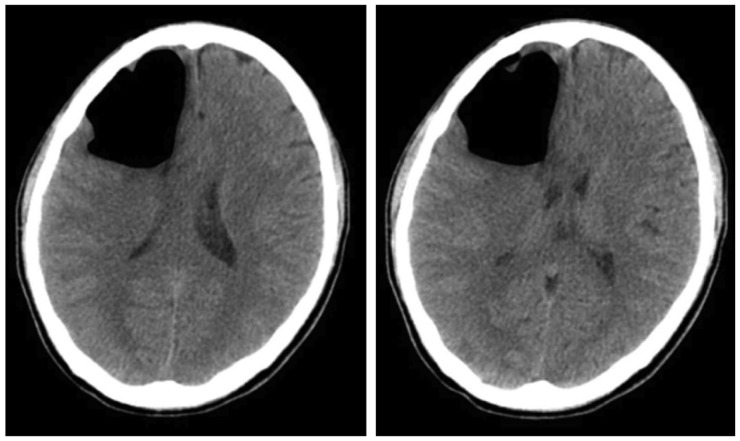
FIGURE 1 Newly developed a large amount of pneumocephali at the right frontal lobe with mild mass effect, compressing the right lateral ventricle and shift in the mid-line on brain computed tomography.
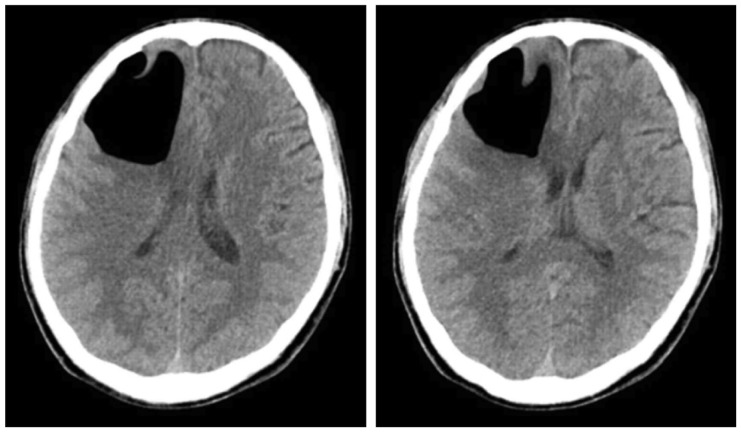
FIGURE 2 This is the last follow-up computed tomography on second admission period; again noted, a large amount of pneumocephali at the right frontal lobe. Mild mass effect, compressing the right lateral ventricle and shift in the mid-line. Little interval changes in the large pneumocephali at the right frontal lobe.
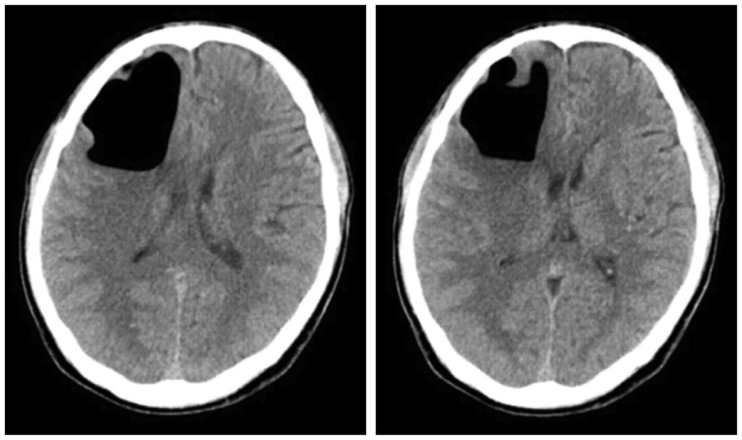
FIGURE 3 Little interval changes in the large pneumocephali at the right frontal lobe on brain computed tomography.
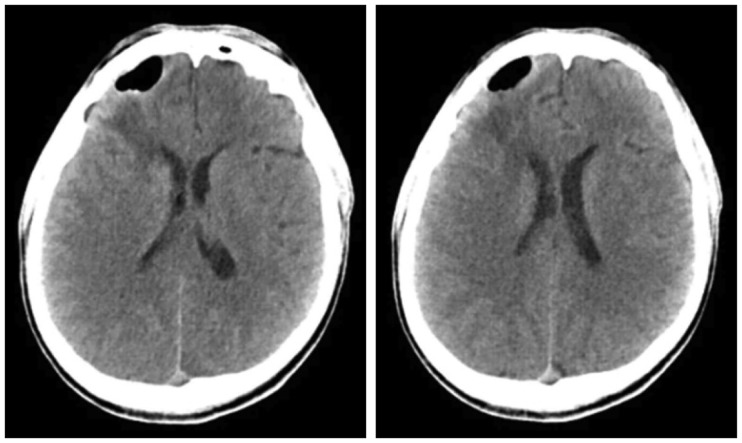
FIGURE 4 Intervally marked decreased intraparenchymal pneumocephalus in right frontal lobe and increased heterogeneous density fluid collection and perilesional low density edema in the cavity of right frontal lobe on brain computed tomography.
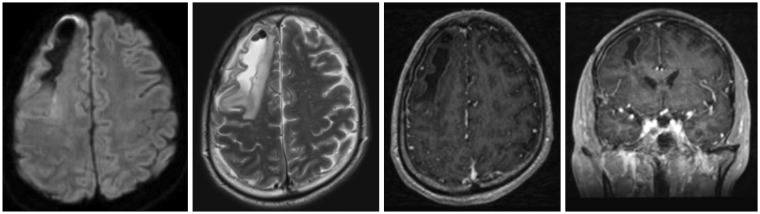
FIGURE 5 About 6.5×1.5 cm sized irregular intraparenchymal fluid collection with air bubbles and perilesional edema in right frontal lobe with mild enhancement along the wall of fluid collection was observed on brain magnetic resonance imaging (MRI) of axial views of the diffusion-weighted, the T2-weighted, the dynamic contrast enhanced of a coronal image, the dynamic contrast enhanced image along the clockwise direction from a left upside figure. It is mean rule out chronic hematoma, differential diagnosis combined early inflammatory change. Also, decreased pneumocephalus was observed on brain MRI enhance.
Reference
-
1. Al-Aieb A, Peralta R, Ellabib M, El-Menyar A, Al-Thani H. Traumatic tension pneumocephalus: Two case reports. Int J Surg Case Rep. 2017; 31:145–149. PMID: 28152490.
Article2. Bakay L, Glasauer FE. Head injury. Boston, MA: Little, Brown;1980.3. Dabdoub CB, Salas G, Silveira Edo N, Dabdoub CF. Review of the management of pneumocephalus. Surg Neurol Int. 2015; 6:155. PMID: 26500801.
Article4. Dandy WE. Pneumocephalus (intracranial pneumatocele or aerocele). Arch Surg. 1926; 12:949–982.5. Eljamel MS, Foy PM. Post-traumatic CSF fistulae, the case for surgical repair. Br J Neurosurg. 1990; 4:479–483. PMID: 2076209.
Article6. Horowitz M. Intracranial pneumocoele. an unusual complication following mastoid surgery. J Laryngol Otol. 1964; 78:128–134. PMID: 14126276.7. Hubbard JL, McDonald TJ, Pearson BW, Laws ER. evolving concepts in diagnosis and surgical management based on the Mayo Clinic experience from 1970 through 1981. Neurosurgery. 1985; 16:314–321. PMID: 3982609.8. Kankane VK, Jaiswal G, Gupta TK. Posttraumatic delayed tension pneumocephalus: Rare case with review of literature. Asian J Neurosurg. 2016; 11:343–347. PMID: 27695534.
Article9. Komolafe EO, Faniran EA. Tension pneumocephalus: A rare but treatable cause of rapid neurological deterioration in traumatic brain injury: A case report. Afr J Neurol Sci. 2010; 29:88–91.10. Kon T, Hondo H, Kohno M, Kasahara K. Severe tension pneumocephalus caused by opening of the frontal sinus by head injury 7 years after initial craniotomy--case report. Neurol Med Chir (Tokyo). 2003; 43:242–245. PMID: 12790283.
Article11. Lunsford LD, Maroon JC, Sheptak PE, Albin MS. Subdural tension pneumocephalus. Report of two cases. J Neurosurg. 1979; 50:525–527. PMID: 423011.13. Park JI, Strelzow VV, Friedman WH. Current management of cerebrospinal fluid rhinorrhea. Laryngoscope. 1983; 93:1294–1300. PMID: 6621228.
Article14. Satapathy GC, Dash HH. Tension pneumocephalus after neurosurgery in the supine position. Br J Anaesth. 2000; 84:115–117. PMID: 10740562.
Article15. Vitali AM, le Roux. A case report. Indian J Neurotrauma. 2007; 4:115–118.
