Cytologic Characteristics of Thymic Adenocarcinoma with Enteric Differentiation: A Study of Four Fine-Needle Aspiration Specimens
- Affiliations
-
- 1Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hanjho@skku.edu
- KMID: 2392571
- DOI: http://doi.org/10.4132/jptm.2017.03.22
Abstract
- Thymic adenocarcinoma is extremely rare. Although its histologic features have been occasionally reported, a lack of description of the cytologic features has hampered the prompt and accurate diagnosis of this condition. Herein, we describe the cytologic findings and histology of four aspiration cytology specimens of thymic adenocarcinoma. The specimens were obtained from primary tumors, metastatic lymph nodes, and pericardial effusions. All four specimens showed three-dimensional glandular clusters with a loss of polarity and nuclear overlapping. One specimen had extensive extracellular mucinous material. Three specimens contained tumor cells with intracytoplasmic vacuoles. While the specimen with extracellular mucin showed relatively mild cytologic atypia, other specimens exhibited more atypical cytologic changes: irregular nuclear membranes, a coarse chromatin pattern, and prominent nucleoli. The cytologic features were correlated with the histologic features in each case of enteric type thymic adenocarcinoma. The differential diagnosis included other thymic carcinomas, yolk sac tumors, and metastatic adenocarcinoma from the lung or colorectum.
Keyword
MeSH Terms
Figure
-
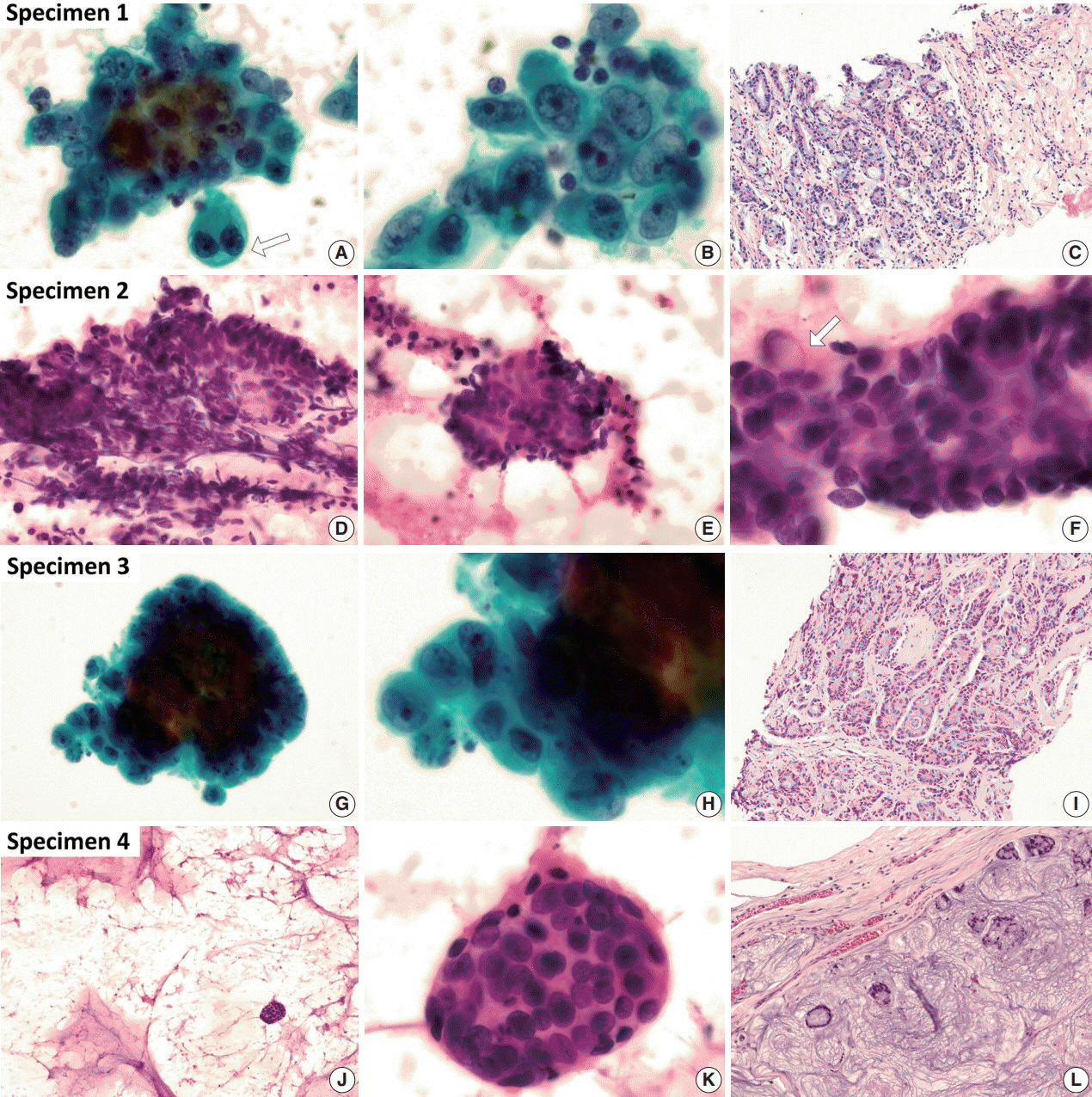
Fig. 1. Cytologic characteristics of thymic adenocarcinoma with histology. (A–C) The fine-needle aspiration (FNA) specimen was obtained from a mediastinal lymph node. Some epithelial cell clusters with a three-dimensional glandular structure are shown. The variably-sized cells have atypical nuclei showing an irregular margin, distinct margination, vesicular chromatin, and prominent nucleoli. Loss of polarity is also present. The cytoplasm is moderately abundant, and intracytoplasmic vacuoles are not infrequently seen (arrow). Adenocarcinoma with a tubular pattern is revealed in the histomorphology of the core biopsy from the tumor. Glandular structure, atypical nuclei, eosinophilic cytoplasm, intracytoplasmic vacuoles, and surrounding inflammatory cells and fibrotic stroma are identical findings with aspiration cytology (A and B, Wright-Giemsa stain). (D–I) Two separate FNAs were carried out in a supraclavicular lymph node (D–F) and the pericardial effusion (G, H). There are glandular- and cribriform-patterned clusters with an inflammatory background. Palisading and stratification are frequently found in clusters. An irregular nuclear margin, vesicular chromatin, prominent nucleoli, and an occasional intracytoplasmic vacuole (arrow) are shown in this sample from patient 2. A core biopsy specimen was obtained from the mediastinal tumor. The tumor shows a tubular and cribriform pattern, stratified nuclei, eosinophilic cytoplasm, intracytoplasmic vacuoles, and inflammatory cells (G and H, Wright-Giemsa stain). (J–L) Most of the aspiration specimen obtained from the tumor is mucinous material. Only a few clusters can be detected. A round cluster of tumor cells reveals relatively mild nuclear atypia. Nuclear overlapping and irregular arrangement are still observed. The excisional specimen reveals floating tumor cells with a tubular or cribriform pattern within the extensive extracellular mucin.
Reference
-
1. Ahmad U, Yao X, Detterbeck F, et al. Thymic carcinoma outcomes and prognosis: results of an international analysis. J Thorac Cardiovasc Surg. 2015; 149:95–100.
Article2. Kwon AY, Han J, Chu J, et al. Histologic characteristics of thymic adenocarcinomas: clinicopathologic study of a nine-case series and a review of the literature. Pathol Res Pract. 2017; 213:106–12.
Article3. Marx A, Chan JK, Coindre JM, et al. The 2015 World Health Organization classification of tumors of the thymus: continuity and changes. J Thorac Oncol. 2015; 10:1383–95.
Article4. Moser B, Schiefer AI, Janik S, et al. Adenocarcinoma of the thymus, enteric type: report of 2 cases, and proposal for a novel subtype of thymic carcinoma. Am J Surg Pathol. 2015; 39:541–8.5. Banki F, Khalil K, Kott MM, Cota AL. Adenoid cystic carcinoma of the thymus gland: a rare tumor. Ann Thorac Surg. 2010; 90:e56–8.
Article6. Furtado A, Nogueira R, Ferreira D, Tente D, Eisele R, Parente B. Papillary adenocarcinoma of the thymus: case report and review of the literature. Int J Surg Pathol. 2010; 18:530–3.
Article7. Zaitlin N, Rozenman J, Yellin A. Papillary adenocarcinoma in a thymic cyst: a pitfall of thoracoscopic excision. Ann Thorac Surg. 2003; 76:1279–81.
Article8. Abdul-Ghafar J, Yong SJ, Kwon W, Park IH, Jung SH. Primary thymic mucinous adenocarcinoma: a case report. Korean J Pathol. 2012; 46:377–81.
Article9. Cho EN, Park HS, Kim TH, et al. A rare case of primary thymic adenocarcinoma mimicking small cell lung cancer. Tuberc Respir Dis. 2015; 78:112–9.
Article10. Jung HY, Cho H, Chung JH, et al. A rare case of primary tubular adenocarcinoma of the thymus, enteric immunophenotype: a case study and review of the literature. J Pathol Transl Med. 2015; 49:331–4.
Article11. Ra YJ, Bae MJ, Kim YS, Choi KU. Difficulties in diagnosis and treatment of thymic adenocarcinoma producing beta-human chorionic gonadotropin in anterior mediastinum. Interact Cardiovasc Thorac Surg. 2010; 11:114–6.12. Seon HJ, Kim KH, Choi YD, et al. Angina pectoris caused by the extrinsic compression of coronary artery by primary thymic mucinous adenocarcinoma. Int J Cardiol. 2012; 156:e13–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fine Needle Aspiration Cytology of Metastatic Prostatic Adenocarcinoma, Pseudohyperplastic Variant
- Fine Needle Aspiration Cytology of Inflammatory Pseudotumor of the Lung: Report of A Case Misdiagnosed as Adenocarcinoma
- Fine Needle Aspiraton Cytology of Polymorphous Low Grade Adenocarcinoma in the Hard Palate: A Case Report
- Fine needle aspiration cytology of malignant thymoma: two cases of invasive thymoma and thymic carcinoma
- Fine Needle Aspiration Cytology of Myxoid Liposarcoma of the Mediastinum
