Perinatology.
2017 Sep;28(3):103-107. 10.14734/PN.2017.28.3.103.
Hypocalvaria of Newborn Infant: Intrauterine Exposure to an Angiotensin Receptor Blocker
- Affiliations
-
- 1Department of Pediatrics, Korea University College of Medicine, Seoul, Korea. sourerkr@korea.ac.kr
- 2Department of Radiology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2392432
- DOI: http://doi.org/10.14734/PN.2017.28.3.103
Abstract
- Angiotensin receptor blockers are contraindicated drugs during pregnancy because of their potential fetotoxicity, including oligohydramnios, anuria, renal tubular dysplasia, limb contractures, cranial ossification defects, prolonged patent ductus arteriosus, and even in utero death. It is believed that these abnormalities are associated with drug-mediated fetal hypotension. We report a case of skull ossification defects, pneumothorax, renal parenchymal disease, congenital calcaneovalgus foot, and inferior vena cava thrombosis in a neonate born to a hypertensive woman who had continued use of an angiotensin receptor blocker during her pregnancy.
MeSH Terms
Figure
-
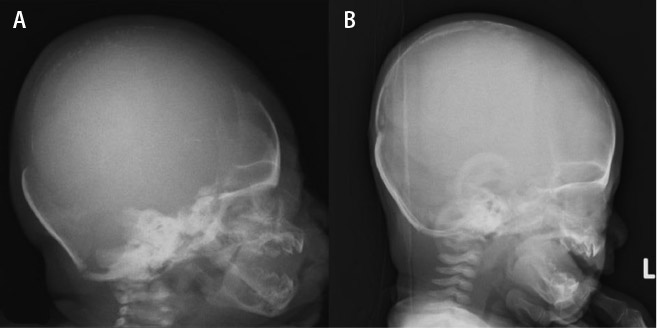
Fig. 1 Left lateral plain skull radiograph. (A) Poor ossification of frontal, temporal, parietal, and occipital bones at birth. (B) Fully developed skull bones at 2 months' of age.
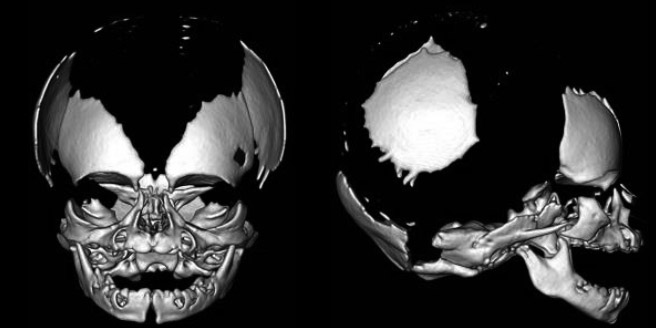
Fig. 2 Three-dimensional computed tomography volume rendering images of the skull showing poor ossification of the frontal, temporal, parietal, and occipital bones. Wide cranial sutures are noted.

Fig. 3 Mild spontaneous pneumothorax is visible on the chest radiograph. The arrows show the pleural line.

Fig. 4 Abdominal computed tomography and inferior vena cavography. Complete obstruction of the iliac vein and inferior vena cava are visible. The arrow shows the thrombus of the inferior vena cava.
Reference
-
1. Diav-Citrin O, Shechtman S, Halberstadt Y, Finkel-Pekarsky V, Wajnberg R, Arnon J, et al. Pregnancy outcome after in utero exposure to angiotensin converting enzyme inhibitors or angiotensin receptor blockers. Reprod Toxicol. 2011; 31:540–545.
Article2. Pryde PG, Sedman AB, Nugent CE, Barr M Jr. Angiotensin-converting enzyme inhibitor fetopathy. J Am Soc Nephrol. 1993; 3:1575–1582.
Article3. Easterling TR, Carr DB, Davis C, Diederichs C, Brateng DA, Schmucker B. Low-dose, short-acting, angiotensin-converting enzyme inhibitors as rescue therapy in pregnancy. Obstet Gynecol. 2000; 96:956–961.
Article4. Boix E, Zapater P, Picó A, Moreno O. Teratogenicity with angiotensin II receptor antagonists in pregnancy. J Endocrinol Invest. 2005; 28:1029–1031.
Article5. Barr M Jr. Teratogen update: angiotensin-converting enzyme inhibitors. Teratology. 1994; 50:399–409.
Article6. Barr M Jr, Cohen MM Jr. ACE inhibitor fetopathy and hypocalvaria: the kidney-skull connection. Teratology. 1991; 44:485–495.
Article7. Schaefer C. Angiotensin II-receptor-antagonists: further evidence of fetotoxicity but not teratogenicity. Birth Defects Res A Clin Mol Teratol. 2003; 67:591–594.
Article8. Shotan A, Widerhorn J, Hurst A, Elkayam U. Risks of angiotensin-converting enzyme inhibition during pregnancy: experimental and clinical evidence, potential mechanisms, and recommendations for use. Am J Med. 1994; 96:451–456.
Article9. Seo HJ, Bae SH, Lee KM. Research on pregnancy and childbirth support policy for the promotion of maternal rights for women with disabilities. Korea: Korea Disabled People's Development Institute;2016.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Neonate with Acute Renal Failure after Maternal Treatment with Angiotensin II Receptor Blocker
- Lithium Intoxication Induced by Angiotensin II Receptor Blocker/Thiazide Combination Agent
- Angiotensin II Receptor Blocker Fetopathy with Persistent Pulmonary Hypertension, Hypocalvaria, Nephrogenic Diabetes Insi pidus, Transient Pseudohypoaldosteronism and Polycythemia
- Angiotensin receptor blocker add-on therapy in portal hypertension: To use angiotensin receptor blocker or not to use, that is the question
- Lithium Toxicity during Hypertension Treatment Using Angiotensin II Receptor Blocker in a Patient with Bipolar Disorder
