J Korean Ophthalmol Soc.
2017 Sep;58(9):1110-1114. 10.3341/jkos.2017.58.9.1110.
A Case of Idiopathic Unilateral Abducens Nerve Palsy in an Adolescent Patient
- Affiliations
-
- 1Department of Ophthalmology, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea. mojili914@hanmail.net
- KMID: 2390077
- DOI: http://doi.org/10.3341/jkos.2017.58.9.1110
Abstract
- PURPOSE
To report a case of idiopathic unilateral abducens nerve palsy in an adolescent patient.
CASE SUMMARY
A healthy 14-year-old boy presented with binocular horizontal diplopia that started that same day. He did not have any history of trauma, vaccination or infectious disease and showed no other neurological signs. The best corrected visual acuity of both eyes was 20/20. Slit lamp and fundus examinations revealed no other abnormalities. On the alternative prism cover test, he had 6 prism diopter (PD) esotropia with −1 degree abduction limitation in the left eye. After 1 week, the abduction limitation in the left eye was progressed to −3.5 degrees, so we performed brain imaging. The brain magnetic resonance imaging (MRI) and systemic evaluation (serologic test, cerebrospinal fluid examination) were normal therefore, we suspected idiopathic unilateral abducens nerve palsy. Thus, intravenous steroid injection was started, and the patient was partially recovered after 5 days of treatment. At 5 weeks after presentation, diplopia and abduction limitation in the left eye were completely resolved, and recurrence was not found during the 1 year of follow-up.
CONCLUSIONS
We report a case of progressive idiopathic unilateral abducens nerve palsy in an adolescent which has resolved completely after intravenous steroid treatment in a short period.
Keyword
MeSH Terms
Figure
-
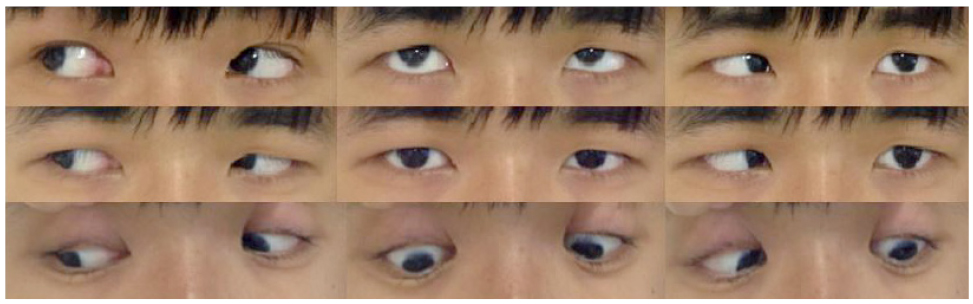
Figure 1 Gaze photographs 1 week after the initial presentation. After 1 week, there was esodeviation with abduction limitation in the left eye.
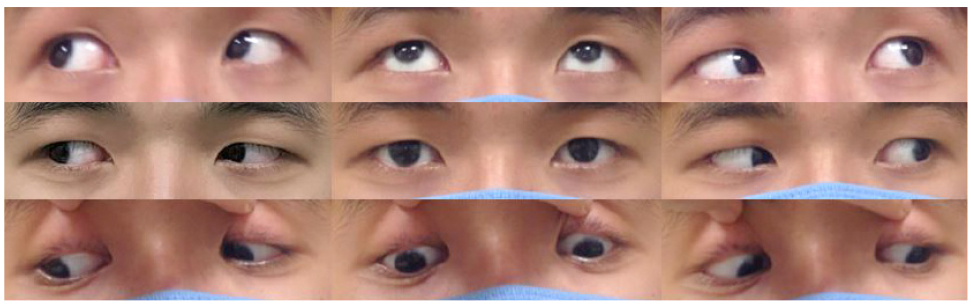
Figure 2 Gaze photographs 4 weeks after the initial presentation. After 4 weeks, there was 4 PD esodeviation of the left eye at left gaze position.
Reference
-
1. Lee MS, Galetta SL, Volpe NJ, Liu GT. Sixth nerve palsies in children. Pediatr Neurol. 1999; 20:49–52.2. Kodsi SR, Young BR. Acquired oculomoter, trochlear, and abducent cranial nerve palsies in pediatric patients. Am J Ophthalmol. 1992; 114:568–574.3. Holmes JM, Mutyala S, Maus TL, et al. Pediatric third, fourth, and sixth nerve palsies: a population-based study. Am J Ophthalmol. 1999; 127:388–392.4. Merino P, Gómez de Liaño P, Villalobo JM, et al. Etiology and treatment of pediatric sixth nerve palsy. J AAPOS. 2010; 14:502–505.5. Richards BW, Jones FR, Young BR. Cause and prognosis in 4,278 cases of paralysis of the oculomotor, trochlear, and abducens cranial nerves. Am J Ophthalmol. 1992; 113:489–496.6. Peters GB 3rd, Bakri SJ, Krohel GB. Cause and prognosis of nontraumatic sixth nerve palsies in young adults. Ophthalmology. 2002; 109:1925–1928.7. Yousuf SJ, Khan AO. Presenting features suggestive for later recurrence of idiopathic sixth nerve paresis in children. J AAPOS. 2007; 11:452–455.8. Afifi AK, Bell WE, Bale JF, Thompson HS. Recurrent lateral rectus palsy in childhood. Pediatr Neurol. 1990; 6:315–318.9. Kim MS, Choi J, Jung JH. Bilateral abducens nerve pasly in peditric patients with Epstein-Barr virus encephalitis. J Korean Ophthalmol Soc. 2013; 54:1303–1308.10. Harley RD. Paralytic strabismus in children. Etiologic incidence and management of the third, fourth, and sixth nerve palsies. Ophthalmology. 1980; 87:24–43.11. Robertson DM, Hines JD, Rucker CW. Acquired sixth-nerve paresis in children. Arch Ophthalmol. 1970; 83:574–579.12. Bet-Shlimon S, Etienne M. Isolated abducens palsy as the first presenting sign of multiple sclerosis. Case Rep Neurol. 2017; 8:272–275.13. Hamilton SR, Lessell S. Recurrent idiopathic lateral rectus muscle palsy in adults. Am J Ophthalmol. 1991; 112:540–542.14. Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell's palsy. N Engl J Med. 2007; 357:1598–1607.15. Yamada K, Kimizu T, Kimura S, et al. Successful treatment with intravenous steroid pulse therapy of a boy with recurrent idiopathic sixth nerve palsy. No To Hattatsu. 2014; 46:287–289.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Isolated Unilateral Abducens Nerve Palsy Caused by Clival Metastasis from Rectal Cancer
- Delayed Bilateral Abducens Nerve Palsy after Head Trauma
- A Case of Benign Abducens Nerve Palsy of Childhood
- Unilateral Abducens Nerve Palsy Associated with Ruptured Anterior Communicating Artery Aneurysm
- Acute unilateral isolated abducens nerve palsy associated with anti-GM1 immunoglobulin M antibody
