Swallowing-Induced Atrial Tachyarrhythmias Successfully Ablated at the Left Posterior Interatrial Septum in Patient with Wolff-Parkinson-White Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. swparkmd@gmail.com
- KMID: 2389135
- DOI: http://doi.org/10.4070/kcj.2015.45.3.253
Abstract
- We reported a case of a 55-year-old patient who presented with palpitation after swallowing. Initial surface electrocardiogram revealed ventricular preexcitation utilizing a left lateral bypass tract. The orthodromic atrioventricular reentrant tachycardia (AVRT) was induced during electrophysiologic studies. After successful ablation of the AVRT utilizing a left lateral free wall bypass tract, 2 different atrial tachycardias (ATs) were induced under isoproterenol infusion. When the patient swallowed saliva or drank water, 2 consecutive beats of atrial premature complexes (APCs) preceded another non-sustained AT repeatedly, which was coincident with the patient's symptom. The preceding APC couplet had the same activation sequence with one induced AT, and the subsequent non-sustained AT had the same activation sequence with the other induced AT, respectively. We first targeted the preceding 2 consecutive APCs at the left posterior interatrial septum. The following non-sustained AT was also eliminated following ablation of the APCs. After ablation, the patient remained free from the swallowing-induced atrial tachyarrhythmias during the one year follow-up.
Keyword
MeSH Terms
Figure
-
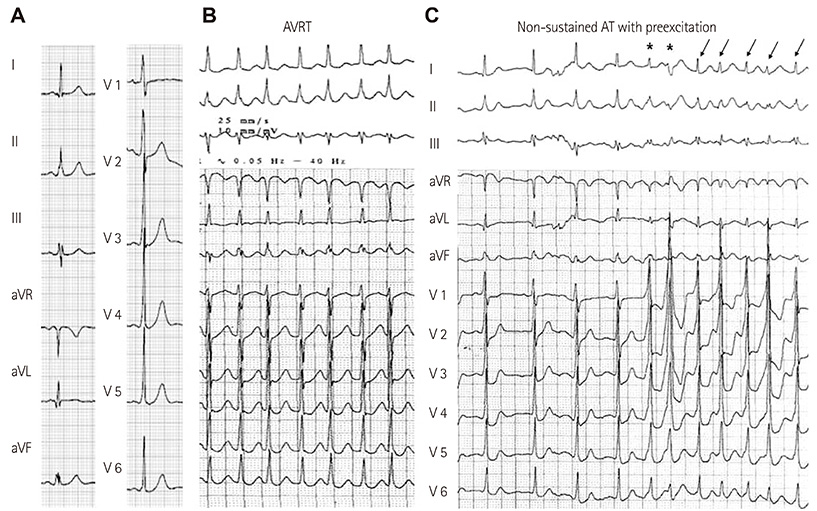
Fig. 1 Baseline 12-lead surface electrocardiogram and clinically documented dual morphology supraventricular tachycardias. A: the delta wave morphology of the Wolff-Parkinson-White syndrome suggests the left lateral free wall bypass tract. B: the narrow regular QRS tachycardia, suggesting atrioventricular reentrant tachycardia (AVRT). C: the short run of irregular atrial tachyarrhythmias with rapid ventricular response related to preexcitation, composed of 2 different types of atrial premature complexes (*) and non-sustained atrial tachycardia (AT, arrows).
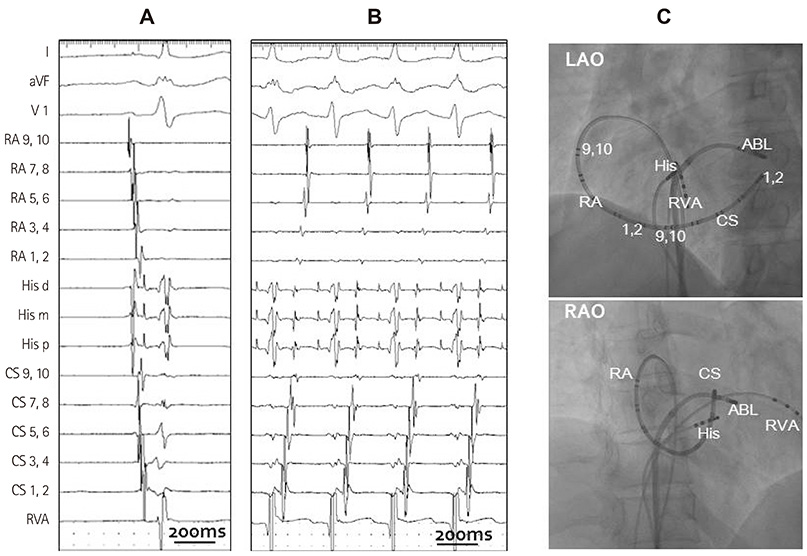
Fig. 2 Wolff-Parkinson-White syndrome and successful ablation site of bypass tract. A: the intra-cardiac electrogram demonstrates the earliest anterograde atrioventricular conduction at the left lateral free wall (CS 1, 2 area). B: atrioventricular reentrant tachycardia demonstrates the earliest retrograde ventriculoatrial conduction at the left lateral free wall (CS 1, 2 area). C: fluoroscopic images in the left anterior oblique (LAO) and right anterior oblique (RAO) projections successful demonstrating the site of the left lateral free wall bypass tract. RA: right atrium, His d: His distal, His m: His middle, His p: His proximal, CS: coronary sinus, RVA: right ventricular apex, ABL: ablation.
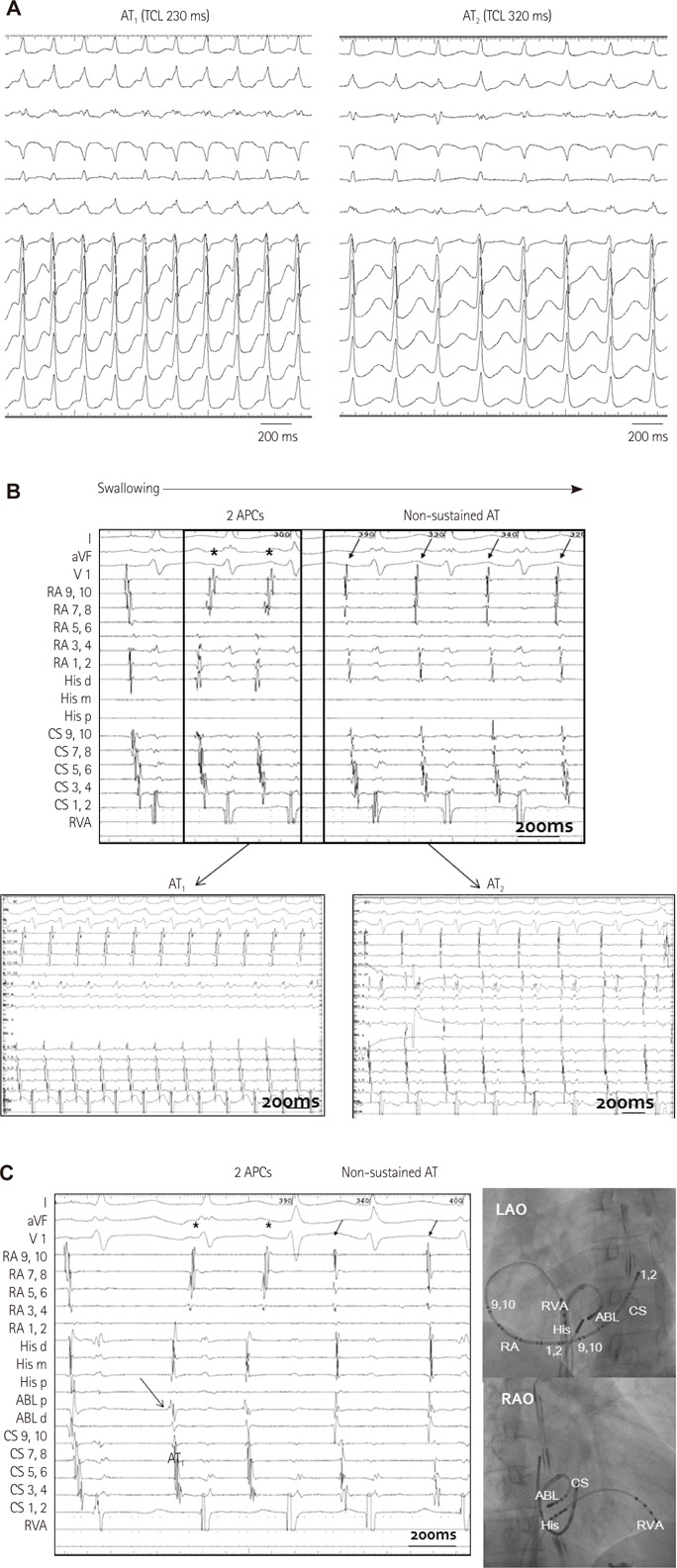
Fig. 3 Swallowing-induced, atrial tachycardias of two different types and successful ablation site. A: 12-lead surface electrocardiogram of two different inducible atrial tachycardias (ATs, AT1, and AT1). B: intra-cardiac electrogram recorded during swallowing. Two consecutive atrial premature complexes (APCs) followed by different morphologies of non-sustained AT (upper panel). Initially induced AT demonstrates the earliest atrial activation of the coronary sinus ostium (CS 9, 10 area) with a cycle length of 230 ms. (AT1, left lower panel). Another morphology of AT demonstrates the earliest atrial activation at the inferior-lateral wall of the tricuspid annulus (RA 5, 6 area) with a cycle length of 320 ms (AT2, right lower panel). C: successful ablation site of swallowing-induced atrial tachyarrhythmias. Electrogram showing the earliest atrial activation site at the left posterior interatrial septum (arrows), preceding the onset of P wave by 25 ms during APCs (left panel). Fluoroscopic images in the left anterior oblique (LAO) and right anterior oblique (RAO) projections, demonstrating the ablation catheter successful positioned at the site on the left posterior interatrial septum (right panel). RA: right atrium, His d: His distal, His m: His middle, His p: His proximal, CS: coronary sinus, RVA: right ventricular apex, ABL: ablation, ABL p: ablation proximal, ABL d: ablation distal.
Reference
-
1. Tada H, Kaseno K, Kubota S, et al. Swallowing-induced atrial tachyarrhythmias: prevalence, characteristics, and the results of the radiofrequency catheter ablation. Pacing Clin Electrophysiol. 2007; 30:1224–1232.2. Greenspon AJ, Volosin KJ. Swallowing-induced tachycardia: electrophysiologic and pharmacologic observations. Pacing Clin Electrophysiol. 1988; 11(11 Pt 1):1566–1570.3. Morady F, Krol RB, Nostrant TT, De Buitleir M, Cline W. Supraventricular tachycardia induced by swallowing: a case report and review of the literature. Pacing Clin Electrophysiol. 1987; 10(1 Pt 1):133–138.4. Matsubara K, Inoue D, Morikawa Y, et al. Swallowing-induced arrhythmia. Clin Cardiol. 1988; 11:798–800.5. Satish OS, Yeh SJ, Yeh KH, et al. Radiofrequency catheter ablation therapy of swallowing-induced atrioventricular nodal reentrant tachycardia: report of two cases. Pacing Clin Electrophysiol. 2005; 28:594–597.6. Yeh SJ, Fu M, Lin FC, Chang CH, Hung JS. Paroxysmal supraventricular tachycardia initiated by a swallowing-induced premature atrial beat. J Electrocardiol. 1986; 19:193–196.7. Baman NS, Baman TS, Taddonio W. Swallowing induced atrial fibrillation. Pacing Clin Electrophysiol. 2004; 27:555–556.8. Yamauchi Y, Aonuma K, Sekiguchi Y, Higuchi K, Obayashi T, Isobe M. Curative therapy for swallowing-induced tachycardia by pulmonary vein antrum isolation. J Cardiovasc Electrophysiol. 2005; 16:1370–1374.9. Yokoshiki H, Mitsuyama H, Watanabe M, Tsutsui H. Swallowing-induced multifocal atrial tachycardia originating from right pulmonary veins. J Electrocardiol. 2011; 44:395.e1–395.e5.10. Undavia M, Sinha S, Mehta D. Radiofrequency ablation of swallowing-induced atrial tachycardia: case report and review of literature. Heart Rhythm. 2006; 3:971–974.11. Nakahara S, Nagashima K, Okumura Y. Proximity relationship between epicardial adipose tissue and the endocardial origin of swallowing-induced atrial tachycardia. Heart Rhythm. 2014; 11:169–170.12. Ardell JL. The cardiac neuronal hierarchy and susceptibility to arrhythmias. Heart Rhythm. 2011; 8:590–591.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left Ventricular Dysfunction and Dilated Cardiomyopathy in Infants and Children with Wolff-Parkinson-White Syndrome in the Absence of Tachyarrhythmias
- Atrial fibrillation in patient with Wolff-Parkinson-White syndrome mimicking ventricular tachycardia
- Spontaneous Transition of Double Tachycardias with Atrial Fusion in a Patient with Wolff-Parkinson-White Syndrome
- Paroxysmal Supraventricular Tachycardia in a Patient with Wolff-Parkinson-White Syndrome Induced by Central Venous Cannulation and Surgical Stimuli during Operation: A case report
- One Case of Cerebral Embolism Associated with Paroxysmal Tachycardia in Wolff-Parkinson-White Syndrome
