Spontaneous Transition of Double Tachycardias with Atrial Fusion in a Patient with Wolff-Parkinson-White Syndrome
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, School of Medicine, Dankook University, Cheonan, Korea. mel_lee@dankook.ac.kr
- KMID: 2344435
- DOI: http://doi.org/10.4070/kcj.2016.46.4.574
Abstract
- Among patients with Wolff-Parkinson-White syndrome, atrioventricular reciprocating tachycardia (AVRT) and atrioventricular nodal reentrant tachycardia (AVNRT) can coexist in a single patient. Direct transition of both tachycardias is rare; however, it can occur after premature atrial or ventricular activity if the cycle lengths of the two tachycardias are similar. Furthermore, persistent atrial activation by an accessory pathway (AP) located outside of the AV node during ongoing AVNRT is also rare. This article describes a case of uncommon atrial activation by an AP during AVNRT and gradual transition of the two supraventricular tachycardias without any preceding atrial or ventricular activity in a patient with preexcitation syndrome.
Keyword
MeSH Terms
Figure
-

Fig. 1 A 12-lead electrocardiogram. Intermittent preexcitation was noted in the late recovery phase during the treadmill test. Delta wave polarity suggested an accessory pathway in the left free wall.
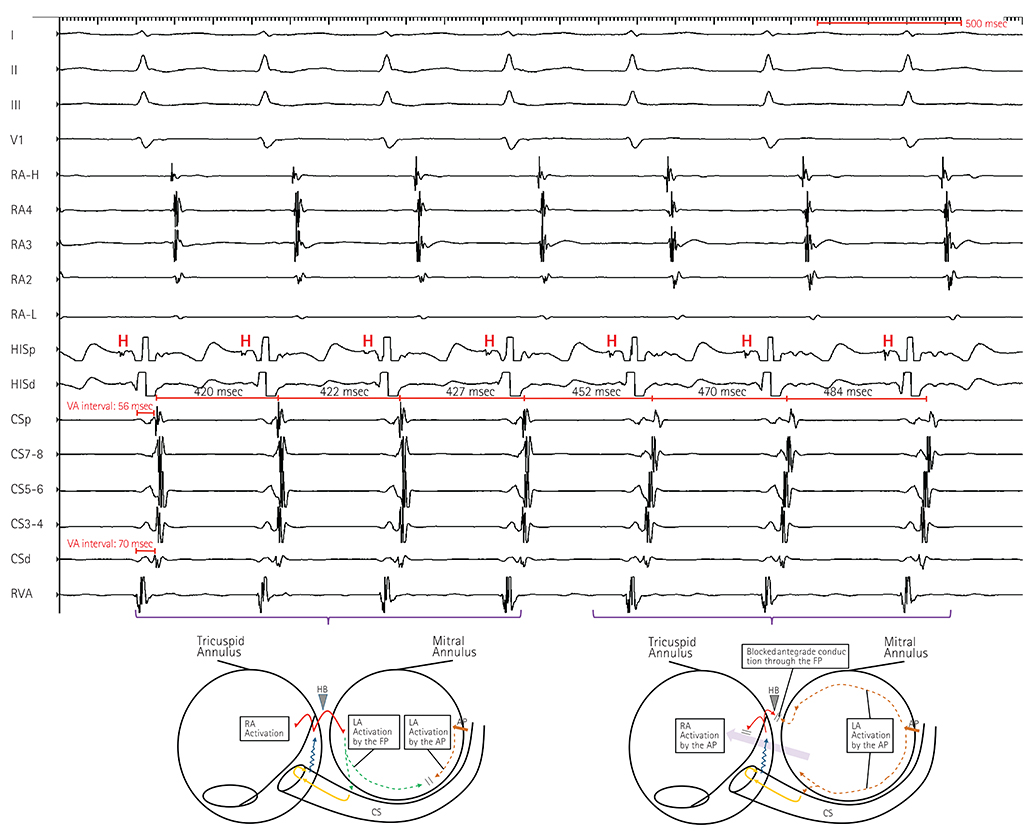
Fig. 2 Induced tachycardia (upper) and schematic drawing of atrial activation (below). Fusion of the sequence of retrograde atrial activation with slight lengthening of the tachycardia CLs, followed by transition to AVRT using the left free wall accessory pathway. The VA interval of 70 msec measured in the distal CS recording was constant. CL: cycle length, AVRT: atrioventricular reciprocating tachycardia, VA: ventriculoatrial, CS: coronary sinus, RA-H: right atrium high, RA-L: right atrium low, HISp: His-bundle electrogram proximal, HISd: His-bundle electrogram distal, CSp: coronary sinus proximal, CSd: coronary sinus distal, RVA: right ventricle apex, LA: left atrium, AP: accessory pathway.

Fig. 3 His-synchronous ventricular extrastimulation. Although the short VA intervals in the proximal CS region suggested AVNRT, atrial activation was advanced (418 msec to 414 msec) with single premature ventricular pacing at a time of His-bundle refractoriness (arrowhead). VA: ventriculoatrial, CS: coronary sinus, AVNRT: atrioventricular nodal reentrant tachycardia.
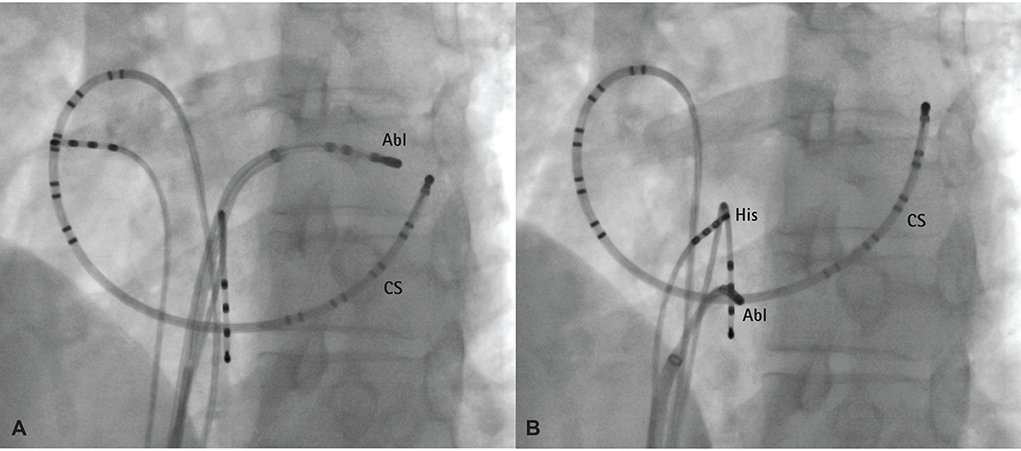
Fig. 4 Fluoroscopic imaging of the ablation site. Left anterior oblique fluoroscopic views of the successful radiofrequency catheter ablation site at the anterolateral aspect of the mitral annulus via a transseptal approach (A) and at the triangle of Koch for slow pathway modulation (B). Abl: ablation catheter, CS: coronary sinus.
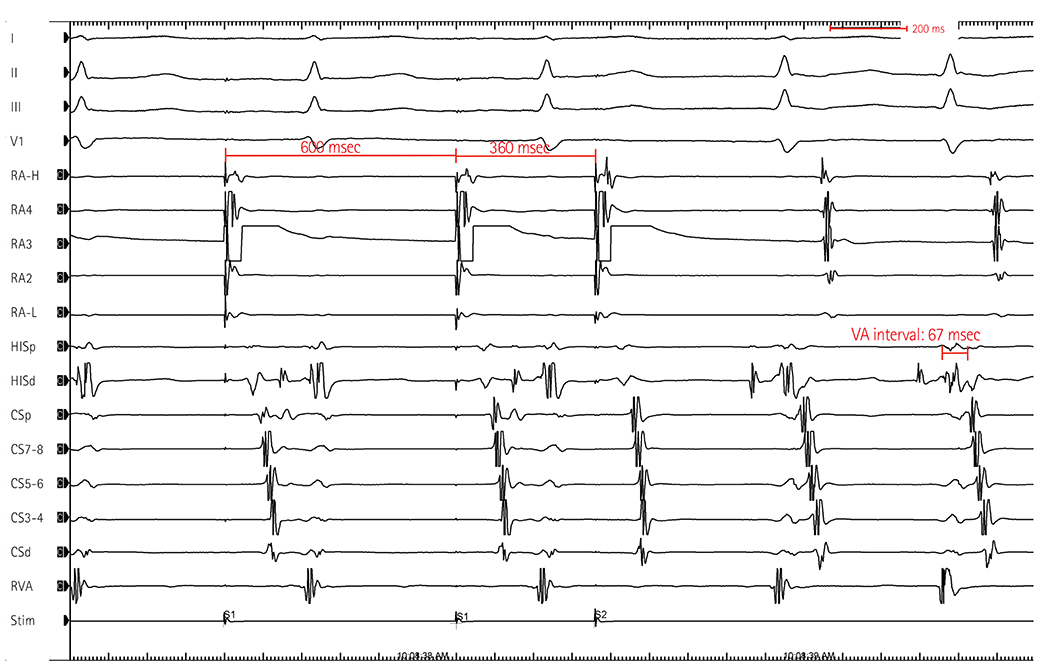
Fig. 5 Induction of tachycardia by single atrial extra-stimulation (A1A2 600/360 msec) after the AP ablation. The retrograde atrial activation sequence was concentric, suggesting typical slow-fast AVNRT. Note splitting of the VA interval in the distal CS recording in comparison with that in Fig. 2. RA-H: right atrium high, RA-L: right atrium low, HISp: His-bundle electrogram proximal, HISd: His-bundle electrogram distal, CSp: coronary sinus proximal, CSd: coronary sinus distal, RVA: right ventricle apex, LA: left atrium, AP: accessory pathway, AVNRT: atrioventricular nodal reentrant tachycardia, VA: ventriculoatrial, CS: coronary sinus.
Reference
-
1. Gallagher JJ, Pritchett EL, Sealy WC, Kasell J, Wallace AG. The preexcitation syndromes. Prog Cardiovasc Dis. 1978; 20:285–327.2. Delacretaz E, Soejima K, Stevenson WG, Friedman PL. Short ventriculoatrial intervals during orthodromic atrioventricular reciprocating tachycardia: what is the mechanism? J Cardiovasc Electrophysiol. 2000; 11:121–124.3. Rakovec P. Transition of orthodromic tachycardia into atrioventricular nodal tachycardia during radiofrequency ablation of an accessory pathway. Europace. 2009; 11:1563–1565.4. Kuo JY, Tai CT, Chiang CE, et al. Mechanisms of transition between double paroxysmal supraventricular tachycardias. J Cardiovasc Electrophysiol. 2001; 12:1339–1345.5. Crawford TC, Mukerji S, Good E, et al. Utility of atrial and ventricular cycle length variability in determining the mechanism of paroxysmal supraventricular tachycardia. J Cardiovasc Electrophysiol. 2007; 18:698–703.6. Hwang C, Martin DJ, Goodman JS, et al. Atypical atrioventricular node reciprocating tachycardia masquerading as tachycardia using a left-sided accessory pathway. J Am Coll Cardiol. 1997; 30:218–225.7. Tada H, Naito S, Taniguchi K, Nogami A. Concealed left anterior accessory pathways: two approaches for successful ablation. J Cardiovasc Electrophysiol. 2003; 14:204–208.8. Luria DM, Nemec J, Etheridge SP, et al. Intra-atrial conduction block along the mitral valve annulus during accessory pathway ablation: evidence for a left atrial "isthmus". J Cardiovasc Electrophysiol. 2001; 12:744–749.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atrial fibrillation in patient with Wolff-Parkinson-White syndrome mimicking ventricular tachycardia
- One Case of Cerebral Embolism Associated with Paroxysmal Tachycardia in Wolff-Parkinson-White Syndrome
- Two Cases of Wolff-Parkinson-White Syndrome in a Family
- Wolff-Parkinson-White Syndrome Treated with Radiofrequency Ablation in Father and His Son
- A Case of Early Onset MELAS Patient with Wolff-Parkinson-White Syndrome
