Multifocal Osteonecrosis in a Patient with Gout: Case Report and Review of the Literature
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Wonkwang University School of Medicine, Iksan, Korea. lch110@wonkwang.ac.kr
- KMID: 2389067
- DOI: http://doi.org/10.4078/jrd.2017.24.4.246
Abstract
- Osteonecrosis (ON) is a common comorbidity in gout; however, avascular ON of multiple sites is unusual. Multifocal ON is defined as osteonecrotic lesions affecting three or more separate anatomic sites. We report a case of a 31-year-old woman diagnosed with gout, who had multifocal ON. Initially, she was treated with benzbromarone, colchicine, and meloxicam. Two years later, she developed severe tophi and was diagnosed with chronic renal failure. Magnetic resonance imaging (MRI) of both legs revealed bilateral ON of the femoral head. She underwent bilateral hip replacement surgeries. After two years, she had pain and limited movements in the left shoulder, with tophi identified via dual-energy computed tomography. Despite management with non-steroidal anti-inflammatory drugs, colchicine, and prednisolone, she had persistent shoulder pain. MRI of the left shoulder revealed ON. She therefore underwent left shoulder replacement surgery. Following the case report, we review the literature on multifocal ON with gout.
Keyword
MeSH Terms
Figure
-
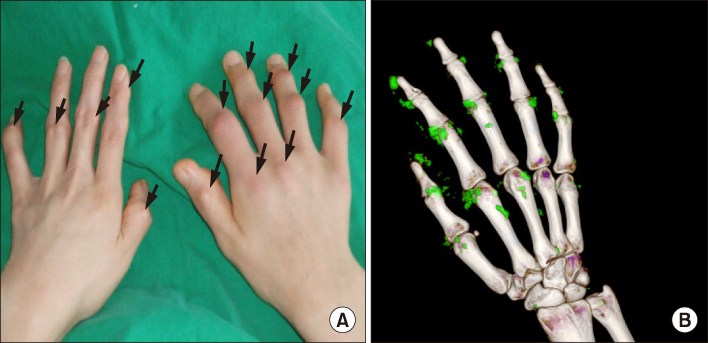
Figure 1 (A) Multiple tophi on both hands (arrows). (B) Dualenergy computed tomography image demonstrating uric acid deposits (green color) on the proximal interphalangeal joints of the right hand.

Figure 2 (A) Anteroposterior hip radiograph showing osteonecrosis of the left hip joint. The left hip joint shows a collapsed femoral head and joint space narrowing compared with the right hip joint (Ficat Stage IV). (B) Intra-operative left hip joint image showing a gout tophi-induced degeneration (arrow). (C) Anteroposterior hip radiograph showing osteonecrosis of the right hip joint.

Figure 3 (A) Anteroposterior left shoulder joint radiograph showing a collapsed deformity with inhomogeneous sclerotic changes in the left humeral head. (B) Dual-energy computed tomography image showing a uric acid deposition in the left acromion. (C) T2-weighted magnetic resonance image of the left shoulder joint. High signal intensity in the humeral head (arrows) suggests a necrotic area. Multiple rounded and oval nodular lesions in the glenohumeral joint with dark signal intensity in all sequences indicate osteophytes (arrowheads). The findings are suggestive of advanced stage of avascular necrosis of the humeral head (Ficat Stage III). (D) T1-weighted magnetic resonance image showing a low signal intensity (arrows), which suggests.
Reference
-
1. Symptomatic multifocal osteonecrosis. A multicenter study. Collaborative Osteonecrosis Group. Clin Orthop Relat Res. 1999; (369):312–326.2. Sattui SE, Singh JA, Gaffo AL. Comorbidities in patients with crystal diseases and hyperuricemia. Rheum Dis Clin North Am. 2014; 40:251–278.3. Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum. 2002; 32:94–124.4. Choi IH, Pizzutillo PD, Bowen JR, Dragann R, Malhis T. Sequelae and reconstruction after septic arthritis of the hip in infants. J Bone Joint Surg Am. 1990; 72:1150–1165.5. Li W, Fan Q, Ma B, Ren M, Li H, Gou Y, et al. [An animal model of Perthes disease and an experimental research of VEGF expression]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008; 22:814–819.6. Calvo-Alén J, Alarcón GS, Tew MB, Tan FK, McGwin G Jr, Fessler BJ, et al. Systemic lupus erythematosus in a multiethnic US cohort: XXXIV. Deficient mannose-binding lectin exon 1 polymorphisms are associated with cerebrovascular but not with other arterial thrombotic events. Arthritis Rheum. 2006; 54:1940–1945.7. Zsernaviczky J, Dressler D. [Gout, pseudo-gout or hyperlipoproteinemia? (author's transl)]. Z Orthop Ihre Grenzgeb. 1976; 114:243–247.8. Orlić D, Jovanović S, Anticević D, Zecević J. Frequency of idiopathic aseptic necrosis in medically treated alcoholics. Int Orthop. 1990; 14:383–386.9. Mauvoisin F, Bernard J, Gemain J. Tomographic aspects of the hips in gout. Rev Rhum Mal Osteoartic. 1955; 22:336–337.10. Mielants H, Veys EM, DeBussere A, van der Jeught J. Avascular necrosis and its relation to lipid and purine metabolism. J Rheumatol. 1975; 2:430–436.11. Kenzora JE. Ischemic necrosis of femoral head. Part I. Accumulative cell stress: a hypothesis for the etiology of idiopathic osteonecrosis. Instr Course Lect. 1983; 32:242–252.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gout of the Hallucal Medial Sesamoid: A Case Report
- Tarsal Tunnel Syndrome Associated with Gout Tophi: A Case Report
- Intratendinous Tophaceous Gout Mimicking Cellulitis after Achilles Tendon Repair
- Multifocal Osteonecrosis
- Mandibular osteonecrosis following herpes zoster infection in the mandibular branch of the trigeminal nerve: a case report and literature review
