Clin Endosc.
2017 May;50(3):250-253. 10.5946/ce.2016.109.
Evaluation and Endoscopic Management of Esophageal Submucosal Tumor
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, CHA University, Seongnam, Korea. cjy6695@dreamwiz.com
- KMID: 2388821
- DOI: http://doi.org/10.5946/ce.2016.109
Abstract
- Submucosal tumors (SMTs) originate from tissues that constitute the submucosal layer and muscularis propria, and are covered by normal mucosa. Esophageal SMTs are rare, accounting for <1% of all esophageal tumors. However, the recent widespread use of endoscopy has led to a rapid increase in incidental detection of SMTs in Korea. Esophageal SMTs are benign in ≥90% of cases, but the possibility of malignancies such as gastrointestinal stromal tumor and malignant leiomyosarcoma still exists. Therefore, patients undergo resection in the presence of symptoms or the possibility of a malignant tumor. For resection of esophageal SMTs, surgical resection was the only option available in case of possible malignancy, but minimally invasive surgery by endoscopic resection is becoming more preferable to surgical resection with the development of endoscopic ultrasonography, endoscopic techniques, and other devices.
MeSH Terms
Figure
-
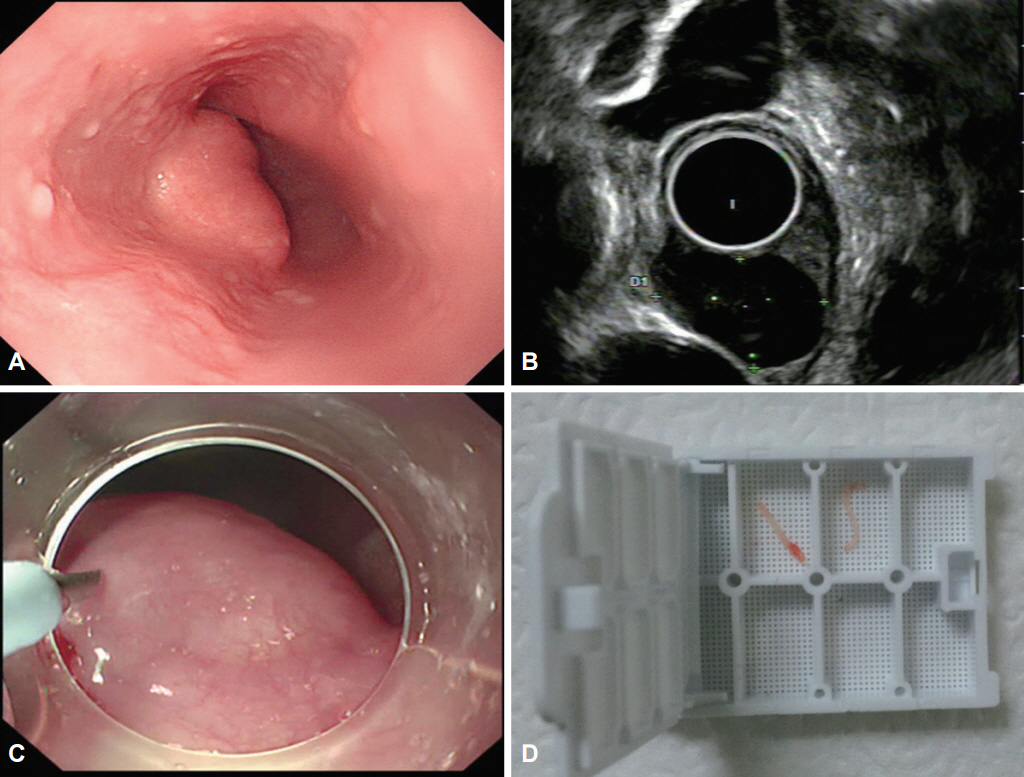
Fig. 1. Tru-Cut biopsy using a flexible endoscope for the diagnosis of submucosal tumor (SMT). (A) SMT observed by using a flexible endoscope. (B) On endoscopic ultrasonography, the SMT is located in the muscularis propria. (C) Tru-Cut biopsy using a flexible endoscope. (D) Specimens.
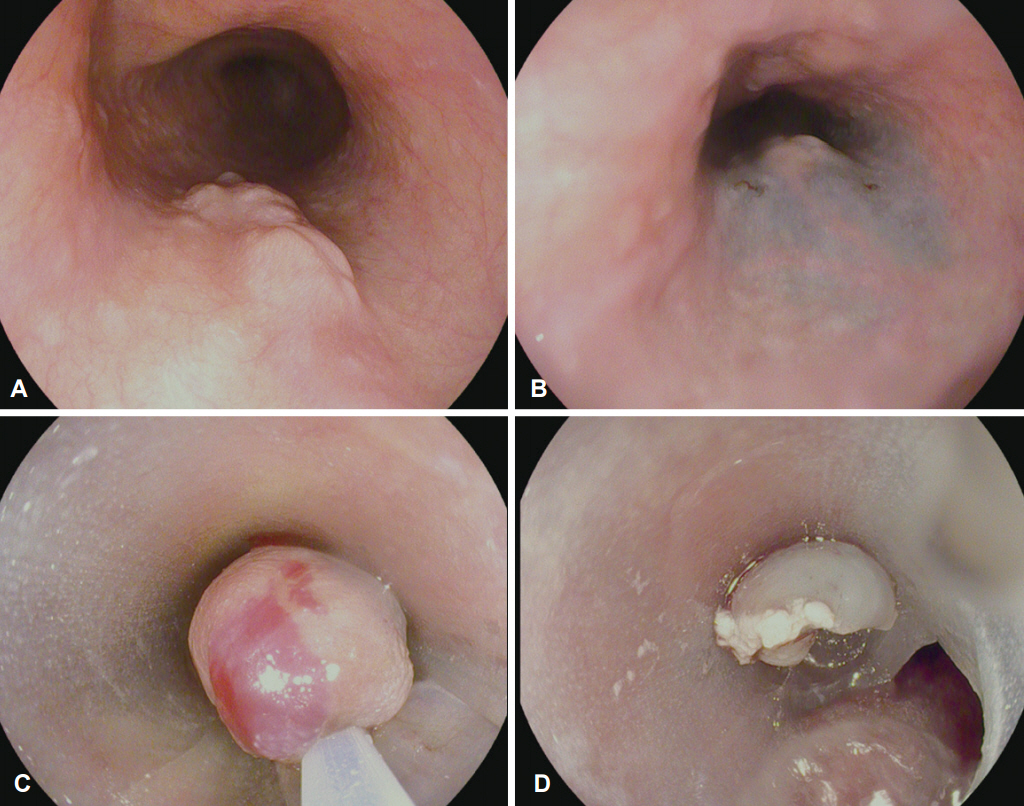
Fig. 2. Application of the three-dimensional printing technique for the side-hole cap during endoscpic mucosal resection with a cap-fitted endoscope applied to a submucosal tumor (SMT). (A) An esophageal SMT. (B) Submucosal injection. (C) Snaring for SMT. (D) Resection of the lesion.
Reference
-
1. Emory TS, Sobin LH, Lukes L, Lee DH, O’Leary TJ. Prognosis of gastrointestinal smooth-muscle (stromal) tumors: dependence on anatomic site. Am J Surg Pathol. 1999; 23:82–87.2. Mutrie CJ, Donahue DM, Wain JC, et al. Esophageal leiomyoma: a 40-year experience. Ann Thorac Surg. 2005; 79:1122–1125.
Article3. Kim MC. Endoscopic incidence of upper gastrointestinal submucosal tumors and endosonographic findings [dissertation]. Suwon: Ajou University School of Medicine;2008.4. Ha TI, Kim GH, Eum JS, et al. Catheter probe endoscopic ultrasonography using the jelly-filled method for esophageal subepithelial lesions. Korean J Gastrointest Endosc. 2008; 36:125–131.5. Gress F, Schmitt C, Savides T, et al. Interobserver agreement for EUS in the evaluation and diagnosis of submucosal masses. Gastrointest Endosc. 2001; 53:71–76.
Article6. Jeong IH, Kim JH, Lee SR, et al. Minimally invasive treatment of gastric gastrointestinal stromal tumors: laparoscopic and endoscopic approach. Surg Laparosc Endosc Percutan Tech. 2012; 22:244–250.7. Mani S, Modlin IM, Ballantyne G, Ahlman H, West B. Carcinoids of the rectum. J Am Coll Surg. 1994; 179:231–248.8. Ko WJ, Song GW, Hahm KB, et al. Tissue diagnosis of GI subepithelial tumor only through Trucut biopsy under a forward-viewing endoscope: applicability as newer diagnostic modality. Surg Endosc. 2016; 30:5009–5014.
Article9. Fujishiro M, Yahagi N, Nakamura M, et al. Successful outcomes of a novel endoscopic treatment for GI tumors: endoscopic submucosal dissection with a mixture of high-molecular-weight hyaluronic acid, glycerin, and sugar. Gastrointest Endosc. 2006; 63:243–249.
Article10. Ko WJ, Song GW, Hong SP, Kwon CI, Hahm KB, Cho JY. Novel 3D-printing technique for caps to enable tailored therapeutic endoscopy. Dig Endosc. 2016; 28:131–138.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Treatment for Esophageal Cancer
- A Submucosal Tumor-Like Recurrence of Early Esophageal Cancer after Endoscopic Submucosal Dissection
- A Case of Esophageal Submucosal Gland Duct Adenoma
- Endoscopic Ultrasonographic Findings of Esophageal Tuberculosis: Case Report
- Submucosal endoscopy: the present and future
