Kosin Med J.
2017 Jun;32(1):105-110. 10.7180/kmj.2017.32.1.105.
A Case of Lactate Containing Peritoneal Dialysis Solution Induced Lactic Acidosis Corrected by Changing to Hemodialysis
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Dong-A University Medical School, Busan, Korea. anws@dau.ac.kr
- KMID: 2384839
- DOI: http://doi.org/10.7180/kmj.2017.32.1.105
Abstract
- Elevated lactate levels are associated with acute illnesses, and the mortality is high. Here, we report a case of lactate-containing peritoneal dialysis (PD) solution inducing lactic acidosis corrected by changing to hemodialysis (HD). This 70-year-old female patient was treated with PD 8 months previously for end-stage renal disease caused by diabetes mellitus. She was admitted complaining of general weakness. Initial lactate level was 22.1 mg/dL and increased to 62.4 mg/dL showing high anion gap metabolic acidosis and compensatory hyperventilation. There are no definite causes of lactic acidosis besides the use of PD solutions containing a lactate component. The patient's lactate level was decreased after temporarily changing the dialysis modality to HD. Her lactate level was increased again after restarting PD, and decreased to normal after restarting HD. We report this case because physicians should consider lactate-containing PD solution as a possible cause of lactic acidosis.
Keyword
MeSH Terms
Figure
-
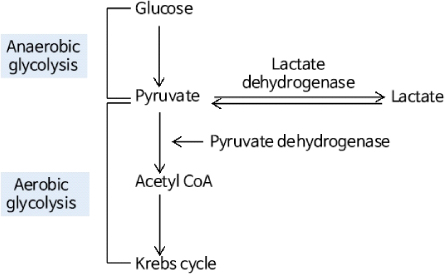
Fig. 1 Summary of lactate metabolism

Fig. 2 Lactate levels according to dialysis modality. After starting hemodialysis (2013.06.11), the lactate level was considerably reduced. After restarting peritoneal dialysis (2015.06.18), the lactate level was increased again. Therefore, we restarted hemodialysis (2015.06.23) and the lactate level was decreased again.
Reference
-
1. Adeva-Andany M, López Ojén M, Funcasta-Calderón R, Ameneiros-Rodriguez E, Donapetry-Garcia C, Vila-Altesor M, et al. Comprehensive review on lactate metabolism in human health. Mitochondrion. 2014; 17:76–100.
Article2. Kraut JA, Madias NE. Lactic acidosis. N Engl J Med. 2014; 371:2309–2319.
Article3. Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate levels. Mayo Clin Proc. 2013; 88:1127–1140.
Article4. Keller G, Cour M, Hernu R, Illinger J, Robert D, Argaud L. Management of metformin-associated lactic acidosis by continuous renal replacement therapy. PLoS One. 2011; 6:e23200.
Article5. Vaziri ND, Ness R, Wellikson L, Barton C, Greep N. Bicarbonate-buffered peritoneal dialysis. An effective adjunct in the treatment of lactic acidosis. Am J Med. 1979; 67:392–396.6. Feriani M. Buffers: bicarbonate, lactate and pyruvate. Kidney Int Suppl. 1996; 56:S75–S80.7. Rachoin JS, Weisberg LS, McFadden CB. Treatment of lactic acidosis: appropriate confusion. J Hosp Med. 2010; 5:E1–E7.
Article8. Kim HJ, Son YK, An WS. Effect of sodium bicarbonate administration on mortality in patients with lactic acidosis: a retrospective analysis. PLoS One. 2013; 8:e65283.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Metformin-Induced Lactic Acidosis Successfully Treated by Hemodialysis
- Clinical Significance of Strong Ion Gap: between ICU and Hemodialysis Patients with Metabolic Acidosis
- Metformin induced acute pancreatitis and lactic acidosis in a patient on hemodialysis
- Three Cases of Mitochondrial Disorders in the Neonatal Period
- A Case of Metformin-Induced Acute Kidney Injury without Lactic Acidosis: A Case Report
