Clinical Implications of Various Criteria for the Biochemical Diagnosis of Insulinoma
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. ymchomd@snu.ac.kr
- KMID: 2384247
- DOI: http://doi.org/10.3803/EnM.2014.29.4.498
Abstract
- BACKGROUND
Among the various diagnostic criteria for insulinoma, the ratio criteria have been controversial. However, the amended insulin-glucose ratio exhibited excellent diagnostic performance in a recent retrospective cohort study, although it has not yet been validated in other patient cohorts. We examined the diagnostic performance of the current criteria of the Endocrine Society, insulin-glucose ratio, C-peptide-glucose ratio, and amended ratios in terms of differentiating insulinomas.
METHODS
We reviewed the medical records of patients who underwent evaluation for hypoglycemia from 2000 to 2013. Fourteen patients with histopathologically confirmed insulinoma and 18 patients without clinical evidence of insulinoma were included. The results of a prolonged fast test were analyzed according to the abovementioned criteria.
RESULTS
Fulfilling all three Endocrine Society criteria-plasma levels of glucose (<3.0 mmol/L), insulin (> or =8 pmol/L), and C-peptide (> or =0.2 nmol/L)-exhibited 100% sensitivity and 89% specificity. Fulfilling the glucose and C-peptide criteria showed 100% sensitivity and 83% specificity, while fulfilling the glucose and insulin criteria showed 100% sensitivity and 72% specificity. Among the ratio criteria, the insulin-glucose ratio [>24.0 (pmol/L)/(mmol/L)] gave the highest area under the receiver operating characteristic curve, with 93% sensitivity and 94% specificity.
CONCLUSION
Fulfilling the glucose, insulin, and C-peptide criteria of the Endocrine Society guidelines exhibited the best diagnostic performance for insulinoma. Nonetheless, the insulin-glucose ratio may still have a role in the biochemical diagnosis of insulinoma.
Keyword
MeSH Terms
Figure
-

Fig. 1 Proportion of patients by time to discontinuation of the prolonged fast test.
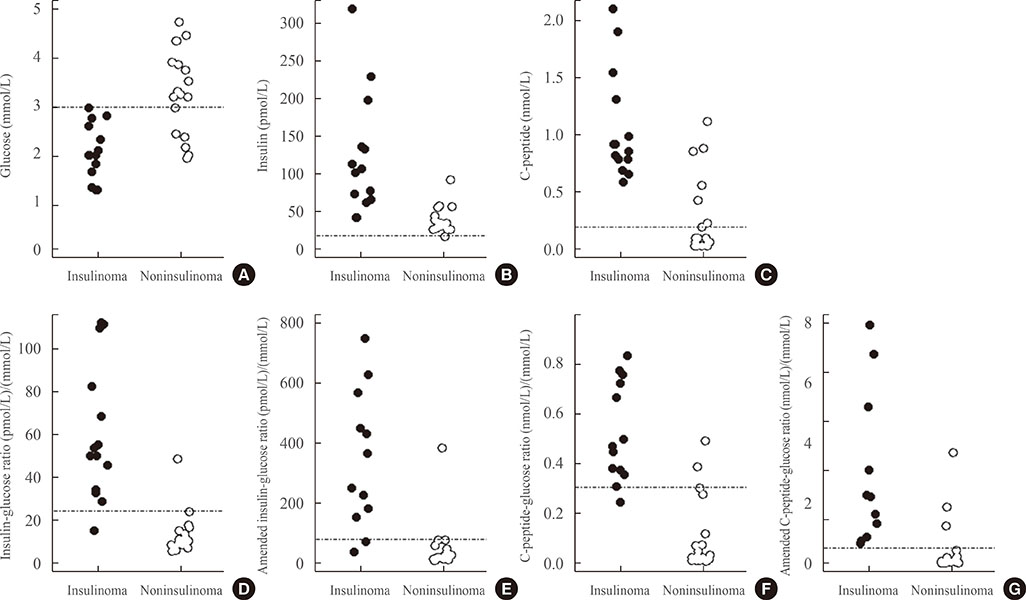
Fig. 2 Distribution of glucose, insulin, C-peptide, insulin-glucose ratio, C-peptide-glucose ratio, amended insulin-glucose ratio, and amended C-peptide-glucose ratio at discontinuation of the prolonged fast test. Scatter plots show the distributions of plasma glucose (A), insulin (B), C-peptide (C), insulin-glucose ratio (D), amended insulin-glucose ratio (E), C-peptide-glucose ratio (F), and amended C-peptide-glucose ratio (G). Dashed lines indicate the cutoff value from the Endocrine Society Clinical Practice Guidelines (A-C) or the cutoff value showing the highest Youden index in the receiver operating characteristic curve analysis of our current data (D-G). Closed circles, insulinoma; open circles, noninsulinoma.
Reference
-
1. Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, Service FJ. Endocrine Society. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009; 94:709–728.2. Grant CS. Insulinoma. Best Pract Res Clin Gastroenterol. 2005; 19:783–798.3. McAuley G, Delaney H, Colville J, Lyburn I, Worsley D, Govender P, Torreggiani WC. Multimodality preoperative imaging of pancreatic insulinomas. Clin Radiol. 2005; 60:1039–1050.4. Placzkowski KA, Vella A, Thompson GB, Grant CS, Reading CC, Charboneau JW, Andrews JC, Lloyd RV, Service FJ. Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007. J Clin Endocrinol Metab. 2009; 94:1069–1073.5. Nauck MA, Meier JJ. Diagnostic accuracy of an "amended" insulin-glucose ratio for the biochemical diagnosis of insulinomas. Ann Intern Med. 2012; 157:767–775.6. Vezzosi D, Bennet A, Fauvel J, Caron P. Insulin, C-peptide and proinsulin for the biochemical diagnosis of hypoglycaemia related to endogenous hyperinsulinism. Eur J Endocrinol. 2007; 157:75–83.7. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine. 18th ed. New York: McGraw-Hill;2012.8. Gardner DG, Shoback DM. Greenspan's basic and clinical endocrinology. 9th ed. New York: McGraw-Hill;2011.9. Turner RC, Oakley NW, Nabarro JD. Control of basal insulin secretion, with special reference to the diagnosis of insulinomas. Br Med J. 1971; 2:132–135.10. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44:837–845.11. Service FJ, Natt N. The prolonged fast. J Clin Endocrinol Metab. 2000; 85:3973–3974.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum: Correction of Figure: Clinical Implications of Various Criteria for the Biochemical Diagnosis of Insulinoma
- Clinical Significance of Hyperinsulinsism - Diagnosis of Insulinoma
- Radiological diagnosis of islet cell tumor: Percutaneous transhepatic portal venous blood sampling
- A Case of Insulinoma without Peripheral Hyperinsulinemia
- A Case of Surgically Treated Insulinoma in Pregnancy
