Ann Pediatr Endocrinol Metab.
2017 Jun;22(2):115-118. 10.6065/apem.2017.22.2.115.
Predictors of transient congenital hypothyroidism in children with eutopic thyroid gland
- Affiliations
-
- 1Department of Pediatrics, Ajou University Hospital, Ajou University School of Medicine, Suwon, Korea. seaon98@naver.com
- KMID: 2383906
- DOI: http://doi.org/10.6065/apem.2017.22.2.115
Abstract
- PURPOSE
Congenital hypothyroidism (CH) is the most common cause of preventable mental retardation. Recently, the detection of CH cases with eutopic thyroid gland has increased due to neonatal screening programs. In this study, we aimed to identify and evaluate predictive factors that could distinguish between permanent and transient CH in patients with eutopic thyroid gland.
METHODS
We retrospectively reviewed 100 children diagnosed with CH and with eutopic thyroid gland. All subjects were treated with levothyroxine and underwent re-evaluation after 3 years of age.
RESULTS
Of the 100 CH patients, 35 (35.0%) were diagnosed with permanent CH (PCH) and 65 (65.0%) were diagnosed with transient CH (TCH). The initial thyroid stimulating hormone levels were significantly lower in the TCH subjects than in PCH subjects. In addition, the mean doses of levothyroxine (µg/kg/day) at the 1st, 2nd, and 3rd year of treatment were significantly lower in subjects with TCH than in PCH subjects with eutopic thyroid gland. Based on the receiver operating characteristic (ROC) curve, the optimal cutoff dose of levothyroxine at 3 years of 2.76 µg/kg/day could predict TCH, and was associated with 87.3% sensitivity and 67.6% specificity, with an area under the ROC curve of 0.769.
CONCLUSION
The levothyroxine dose requirement during treatment period has a predictive role in differentiating TCH from PCH in CH patients with eutopic thyroid gland.
MeSH Terms
Figure
-
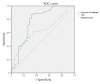
Fig. 1 Receiver operating characteristic (ROC) curves of various thresholds of thyroid stimulating hormone (TSH) (area under the curve [AUC], 0.636; 95% confidence interval [CI], 0.524–0.748) and the levothyroxine dose of 3rd year of treatment (AUC, 0.769; 95% CI, 0.659–0.880) for predicting transient congenital hypothyroidism.
Cited by 2 articles
-
Pediatric thyroid disorders
Young-Lim Shin
J Korean Med Assoc. 2018;61(10):607-615. doi: 10.5124/jkma.2018.61.10.607.Persistent goiter with congenital hypothyroidism due to mutation in
DUOXA2 gene
So Yoon Jung, Jeongho Lee, Dong Hwan Lee
Ann Pediatr Endocrinol Metab. 2020;25(1):57-62. doi: 10.6065/apem.2020.25.1.57.
Reference
-
1. Grüters A, Krude H. Detection and treatment of congenital hypothyroidism. Nat Rev Endocrinol. 2011; 8:104–113. PMID: 22009163.
Article2. LaFranchi SH. Newborn screening strategies for congenital hypothyroidism: an update. J Inherit Metab Dis. 2010; 33(Suppl 2):S225–S233. PMID: 20195902.
Article3. Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis. 2010; 5:17. PMID: 20537182.
Article4. Barry Y, Bonaldi C, Goulet V, Coutant R, Léger J, Paty AC, et al. Increased incidence of congenital hypothyroidism in France from 1982 to 2012: a nationwide multicenter analysis. Ann Epidemiol. 2016; 26:100–105. e1–e4. PMID: 26775052.
Article5. Olivieri A, Corbetta C, Weber G, Vigone MC, Fazzini C, Medda E, et al. Congenital hypothyroidism due to defects of thyroid development and mild increase of TSH at screening: data from the Italian National Registry of infants with congenital hypothyroidism. J Clin Endocrinol Metab. 2013; 98:1403–1408. PMID: 23443814.
Article6. Wassner AJ, Brown RS. Congenital hypothyroidism: recent advances. Curr Opin Endocrinol Diabetes Obes. 2015; 22:407–412. PMID: 26313902.7. Léger J, Olivieri A, Donaldson M, Torresani T, Krude H, van Vliet G, et al. European Society for Paediatric Endocrinology consensus guidelines on screening, diagnosis, and management of congenital hypothyroidism. Horm Res Paediatr. 2014; 81:80–103. PMID: 24662106.
Article8. Messina MF, Aversa T, Salzano G, Zirilli G, Sferlazzas C, De Luca F, et al. Early discrimination between transient and permanent congenital hypothyroidism in children with eutopic gland. Horm Res Paediatr. 2015; 84:159–164. PMID: 26160341.
Article9. Cho MS, Cho GS, Park SH, Jung MH, Suh BK, Koh DG. Earlier re-evaluation may be possible in pediatric patients with eutopic congenital hypothyroidism requiring lower L-thyroxine doses. Ann Pediatr Endocrinol Metab. 2014; 19:141–145. PMID: 25346918.
Article10. Rabbiosi S, Vigone MC, Cortinovis F, Zamproni I, Fugazzola L, Persani L, et al. Congenital hypothyroidism with eutopic thyroid gland: analysis of clinical and biochemical features at diagnosis and after re-evaluation. J Clin Endocrinol Metab. 2013; 98:1395–1402. PMID: 23426615.
Article11. Akobeng AK. Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr. 2007; 96:644–647. PMID: 17376185.
Article12. Ghasemi M, Hashemipour M, Hovsepian S, Heiydari K, Sajadi A, Hadian R, et al. Prevalence of transient congenital hypothyroidism in central part of Iran. J Res Med Sci. 2013; 18:699–703. PMID: 24379847.13. Eugster EA, LeMay D, Zerin JM, Pescovitz OH. Definitive diagnosis in children with congenital hypothyroidism. J Pediatr. 2004; 144:643–647. PMID: 15127002.
Article14. Lim HK, Kim KH, Kim SH, No HY, Kim CJ, Woo YJ, et al. Predictors of transient hypothyroidism in neonatal screening test. J Korean Soc Pediatr Endocrinol. 2006; 11:50–56.15. Hong SY, Chung HR, Lee SY, Shin CH, Yang SW. Factors distinguishing between transient and permanent hypothyroidism in patients diagnosed as congenital hypothyroidism by newborn screening. J Korean Soc Pediatr Endocrinol. 2005; 10:154–160.16. Skordis N, Toumba M, Savva SC, Erakleous E, Topouzi M, Vogazianos M, et al. High prevalence of congenital hypothyroidism in the Greek Cypriot population: results of the neonatal screening program 1990-2000. J Pediatr Endocrinol Metab. 2005; 18:453–461. PMID: 15921174.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypothyroidism
- Changes of antithroglobulin antibody in children with congenital hypothyroidism
- Predictors of Transient Hypothyroidism in Neonatal Screening Test
- Earlier re-evaluation may be possible in pediatric patients with eutopic congenital hypothyroidism requiring lower L-thyroxine doses
- Characteristics of Transient Hypothyroidism Detected by Neonatal Screening Test
