Real-time Vessel Navigation Using Indocyanine Green Fluorescence during Robotic or Laparoscopic Gastrectomy for Gastric Cancer
- Affiliations
-
- 1Department of Surgery, Ajou University School of Medicine, Suwon, Korea. spy798@gmail.com
- KMID: 2383737
- DOI: http://doi.org/10.5230/jgc.2017.17.e17
Abstract
- PURPOSE
Identification of the infrapyloric artery (IPA) type is a key component of pylorus-preserving gastrectomy. As the indocyanine green (ICG) fluorescence technique is known to help visualize blood vessels and flow during reconstruction, we speculated that this emerging technique would be helpful in identifying the IPA type.
MATERIALS AND METHODS
From August 2015 to February 2016, 20 patients who underwent robotic or laparoscopic gastrectomy were prospectively enrolled. After intravenous injection of approximately 3 mL of ICG (2.5 mg/mL), a near-infrared fluorescence apparatus was applied. The identified shape of the IPA was confirmed by examining the actual anatomy following infrapyloric dissection.
RESULTS
The mean interval time between ICG injection and visualization of the artery was 22.2 seconds (range, 14-30 seconds), and the mean duration of the arterial phase was 16.1 seconds (range, 9-30 seconds). The overall positive predictive value (PPV) of ICG fluorescence in identifying the IPA type was 80% (16/20). The IPA type was incorrectly predicted in four patients, all of whom were obese with a body mass index (BMI) of more than 25 kg/m².
CONCLUSIONS
Our preliminary results indicate that intraoperative vascular imaging using the ICG fluorescence technique may be helpful for robotic or laparoscopic pylorus-preserving gastrectomy.
MeSH Terms
Figure
-
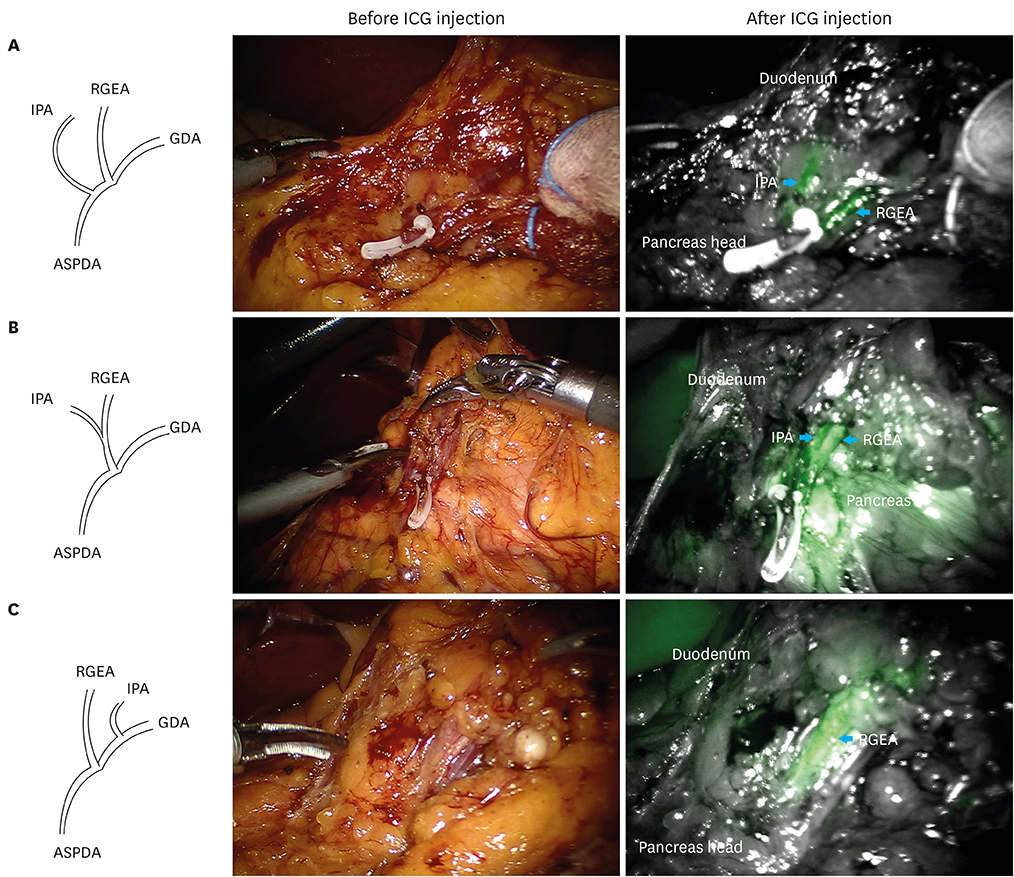
Fig. 1 ICG fluorescence images of various IPA types and an accessory splenic artery. (A) In the distal type, 2 separated fluorescent streams (blue arrows) arise from the pancreas head. (B) In the caudal type, a stream is divided into 2 (blue arrows) at the RGEA. (C) In the proximal type, the duodenum is slightly visualized without any vessel visualization, and then the RGEA is solely visualized (blue arrow). IPA = infrapyloric artery; RGEA = right gastroepiploic artery; GDA = gastroduodenal artery; ASPDA = anterior superior pancreaticoduodenal artery; ICG = indocyanine green.
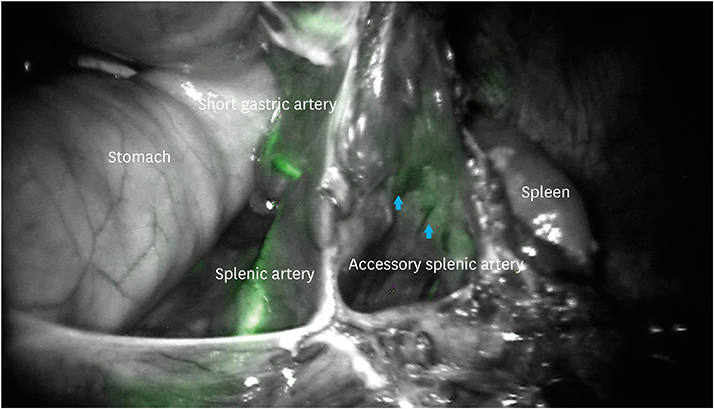
Fig. 2 An accessory splenic artery (blue arrows) from the LGEA. LGEA = left gastroepiploic artery.
Cited by 1 articles
-
Assessment of the Completeness of Lymph Node Dissection Using Near-infrared Imaging with Indocyanine Green in Laparoscopic Gastrectomy for Gastric Cancer
Tae-Han Kim, Seong-Ho Kong, Ji-Ho Park, Yong-Gil Son, Yeon-Ju Huh, Yun-Suhk Suh, Hyuk-Joon Lee, Han-Kwang Yang
J Gastric Cancer. 2018;18(2):161-171. doi: 10.5230/jgc.2018.18.e19.
Reference
-
1. Yada T, Yokoi C, Uemura N. The current state of diagnosis and treatment for early gastric cancer. Diagn Ther Endosc. 2013; 2013:241320.2. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77.3. Isozaki H, Matsumoto S, Murakami S, Takama T, Sho T, Ishihara K, et al. Diminished gastric resection preserves better quality of life in patients with early gastric cancer. Acta Med Okayama. 2016; 70:119–130.4. Ronellenfitsch U, Najmeh S, Andalib A, Perera RM, Rousseau MC, Mulder DS, et al. Functional outcomes and quality of life after proximal gastrectomy with esophagogastrostomy using a narrow gastric conduit. Ann Surg Oncol. 2015; 22:772–779.5. Fujita J, Takahashi M, Urushihara T, Tanabe K, Kodera Y, Yumiba T, et al. Assessment of postoperative quality of life following pylorus-preserving gastrectomy and Billroth-I distal gastrectomy in gastric cancer patients: results of the nationwide postgastrectomy syndrome assessment study. Gastric Cancer. 2016; 19:302–311.6. Xiao XM, Gaol C, Yin W, Yu WH, Qi F, Liu T. Pylorus-preserving versus distal subtotal gastrectomy for surgical treatment of early gastric cancer: a meta-analysis. Hepatogastroenterology. 2014; 61:870–879.7. Jiang X, Hiki N, Nunobe S, Fukunaga T, Kumagai K, Nohara K, et al. Long-term outcome and survival with laparoscopy-assisted pylorus-preserving gastrectomy for early gastric cancer. Surg Endosc. 2011; 25:1182–1186.8. Suh YS, Han DS, Kong SH, Kwon S, Shin CI, Kim WH, et al. Laparoscopy-assisted pylorus-preserving gastrectomy is better than laparoscopy-assisted distal gastrectomy for middle-third early gastric cancer. Ann Surg. 2014; 259:485–493.9. Haruta S, Shinohara H, Ueno M, Udagawa H, Sakai Y, Uyama I. Anatomical considerations of the infrapyloric artery and its associated lymph nodes during laparoscopic gastric cancer surgery. Gastric Cancer. 2015; 18:876–880.10. Yoshida M, Kubota K, Kuroda J, Ohta K, Nakamura T, Saito J, et al. Indocyanine green injection for detecting sentinel nodes using color fluorescence camera in the laparoscopy-assisted gastrectomy. J Gastroenterol Hepatol. 2012; 27:Suppl 3. 29–33.11. Fujita T, Seshimo A, Kameoka S. Detection of sentinel nodes in gastric cancer by indocyanine green fluorescence imaging. Hepatogastroenterology. 2012; 59:2213–2216.12. Tajima Y, Yamazaki K, Masuda Y, Kato M, Yasuda D, Aoki T, et al. Sentinel node mapping guided by indocyanine green fluorescence imaging in gastric cancer. Ann Surg. 2009; 249:58–62.13. Rino Y, Yukawa N, Sato T, Yamamoto N, Tamagawa H, Hasegawa S, et al. Visualization of blood supply route to the reconstructed stomach by indocyanine green fluorescence imaging during esophagectomy. BMC Med Imaging. 2014; 14:18.14. Murawa D, Hünerbein M, Spychała A, Nowaczyk P, Połom K, Murawa P. Indocyanine green angiography for evaluation of gastric conduit perfusion during esophagectomy--first experience. Acta Chir Belg. 2012; 112:275–280.15. Arichi N, Mitsui Y, Ogawa K, Nagami T, Nakamura S, Hiraoka T, et al. Intraoperative fluorescence vascular imaging using indocyanine green for assessment of transplanted kidney perfusion. Transplant Proc. 2014; 46:342–345.16. World Health Organization Western Pacific Region. International Association for the Study of Obesity. International Obesity Task Force. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Sydney: Health Communications Australia Pty Limited;2000.17. Kim YM, Baek SE, Lim JS, Hyung WJ. Clinical application of image-enhanced minimally invasive robotic surgery for gastric cancer: a prospective observational study. J Gastrointest Surg. 2013; 17:304–312.18. Herrera-Almario G, Patane M, Sarkaria I, Strong VE. Initial report of near-infrared fluorescence imaging as an intraoperative adjunct for lymph node harvesting during robot-assisted laparoscopic gastrectomy. J Surg Oncol. 2016; 113:768–770.19. Miyashiro I, Kishi K, Yano M, Tanaka K, Motoori M, Ohue M, et al. Laparoscopic detection of sentinel node in gastric cancer surgery by indocyanine green fluorescence imaging. Surg Endosc. 2011; 25:1672–1676.20. Kim MC, Choi HJ, Jung GJ, Kim HH. Techniques and complications of laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer. Eur J Surg Oncol. 2007; 33:700–705.21. Kim S, Lim YT, Soltesz EG, De Grand AM, Lee J, Nakayama A, et al. Near-infrared fluorescent type II quantum dots for sentinel lymph node mapping. Nat Biotechnol. 2004; 22:93–97.22. Homma S, Fukunaga T, Kagaya A. Influence of adipose tissue thickness on near infrared spectroscopic signal in the measurement of human muscle. J Biomed Opt. 1996; 1:418–424.23. Feng W, Haishu D, Fenghua T, Jun Z, Qing X, Xianwu T. Influence of overlying tissue and probe geometry on the sensitivity of a near-infrared tissue oximeter. Physiol Meas. 2001; 22:201–208.24. Marshall MV, Rasmussen JC, Tan IC, Aldrich MB, Adams KE, Wang X, et al. Near-infrared fluorescence imaging in humans with indocyanine green: a review and update. Open Surg Oncol J. 2010; 2:12–25.25. Ishizawa T, Fukushima N, Shibahara J, Masuda K, Tamura S, Aoki T, et al. Real-time identification of liver cancers by using indocyanine green fluorescent imaging. Cancer. 2009; 115:2491–2504.26. Miyata A, Ishizawa T, Kamiya M, Shimizu A, Kaneko J, Ijichi H, et al. Photoacoustic tomography of human hepatic malignancies using intraoperative indocyanine green fluorescence imaging. PLoS One. 2014; 9:e112667.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Indocyanine green and near-infrared fluorescenceguided surgery for gastric cancer: a narrative review
- Clinical Feasibility of Vascular Navigation System During Laparoscopic Gastrectomy for Gastric Cancer: A Retrospective Comparison With Propensity-Score Matching
- Application of Near-Infrared Fluorescence Imaging with Indocyanine Green in Totally Laparoscopic Distal Gastrectomy
- Robotic Gastrectomy for Gastric Cancer: A Review of Postoperative and Oncologic Outcomes
- Current status of robotic gastrectomy for gastric cancer: A review of recent randomized controlled trials
