Korean J Gastroenterol.
2016 Nov;68(5):260-264. 10.4166/kjg.2016.68.5.260.
Eradication Rate by Duration of Third-line Rescue Therapy with Levofloxacin after Helicobacter pylori Treatment Failure in Clinical Practice
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon, Korea. sjhong@schmc.ac.kr
- 2Digestive Disease Center and Research Institute, Soonchunhyang University College of Medicine, Bucheon, Korea.
- KMID: 2383503
- DOI: http://doi.org/10.4166/kjg.2016.68.5.260
Abstract
- BACKGROUND/AIMS
This study evaluated the eradication rate of levofloxacin-containing rescue therapy by treatment duration in patients in whom previous first- and second-line treatment failed.
METHODS
Fifty-five patients with persistent Helicobacter pylori infection after first-line therapy and second-line therapy were studied in a single referral academic center. We compared the eradication rates by the treatment duration of third-line therapy.
RESULTS
Of 55 patients, 12 (21.8%) received rescue therapy for seven days, 24 (43.6%) received rescue therapy for 10 days, and 19 (34.5%) received rescue therapy for 14 days. The eradication rates of therapy with levofloxacin were 65.5% in the 55 enrolled patients and 73.5% in the 49 patients who underwent follow-up testing. In cases where follow-up testing was performed, the eradication rate of 7-day therapy was 58.3%, of 10-day 68.2%, and of 14-day therapy 93.3%. Eradication rate of 14-day therapy was higher than 7-day (p=0.06) and 10-day (p=0.108), but chance could not be ruled out in the difference among groups.
CONCLUSIONS
This study showed somewhat increasing of H. pylori eradication rate by extending the duration of levofloxacin-containing rescue therapy to 14 days.
Keyword
MeSH Terms
Figure
-
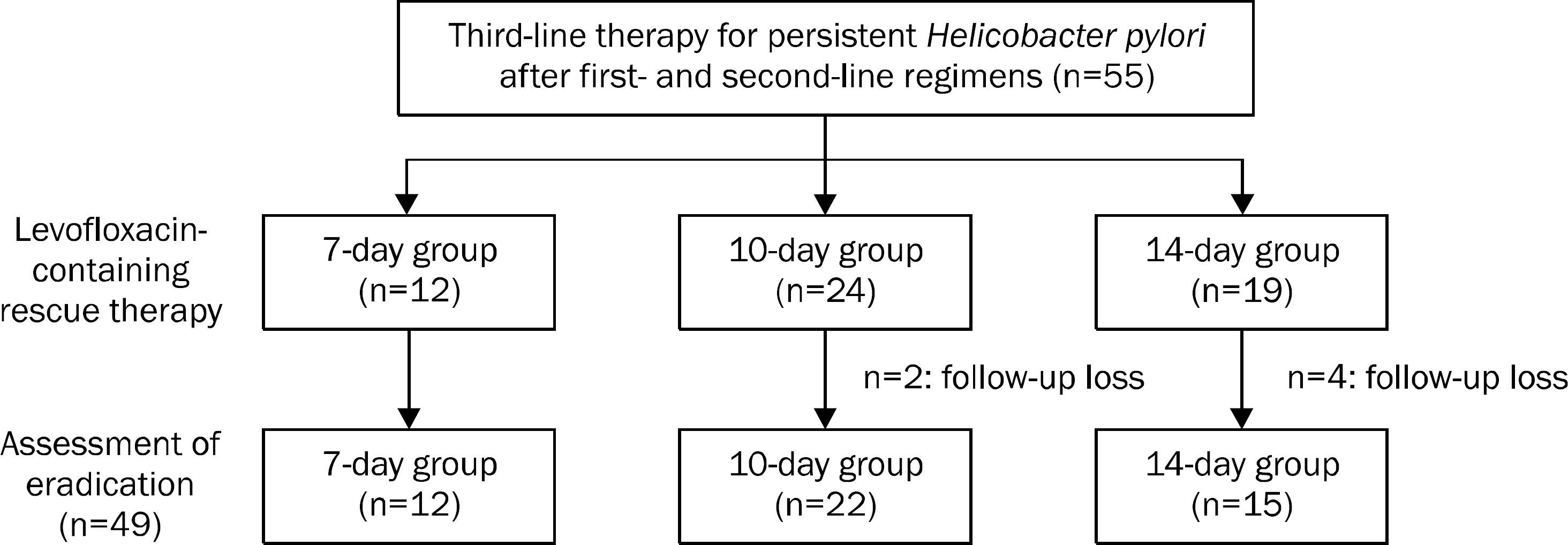
Fig. 1. Study flowchart.
Reference
-
References
1. Graham DY, Fischbach L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut. 2010; 59:1143–1153.2. Lee JW, Kim N, Kim JM, et al. Prevalence of primary and secondary antimicrobial resistance of Helicobacter pylori in Korea from 2003 through 2012. Helicobacter. 2013; 18:206–214.3. An B, Moon BS, Kim H, et al. Antibiotic resistance in Helicobacter pylori strains and its effect on H. pylori eradication rates in a single center in Korea. Ann Lab Med. 2013; 33:415–419.4. Yoon KH, Park SW, Lee SW, Kim BJ, Kim JG. Clarithromycin-based standard triple therapy can still be effective for Helicobacter pylori eradication in some parts of the Korea. J Korean Med Sci. 2014; 29:1240–1246.5. Malfertheiner P, Megraud F, O'Morain CA, et al. Management of Helicobacter pylori infection–the Maastricht IV/Florence Consensus Report. Gut. 2012; 61:646–664.6. Kim SG, Jung HK, Lee HL, et al. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. J Gastroenterol Hepatol. 2014; 29:1371–1386.7. Papastergiou V, Georgopoulos SD, Karatapanis S. Current and future insights in H. pylori eradication regimens: the need of tailoring therapy. Curr Pharm Des. 2014; 20:4521–4532.8. Miehlke S, Krasz S, Schneider-Brachert W, et al. Randomized trial on 14 versus 7 days of esomeprazole, moxifloxacin, and amoxicillin for second-line or rescue treatment of Helicobacter pylori infection. Helicobacter. 2011; 16:420–426.9. Chuah SK, Tai WC, Hsu PI, et al. The efficacy of second-line an-ti-Helicobacter pylori therapy using an extended 14-day levofloxacin/amoxicillin/proton-pump inhibitor treatment-a pilot study. Helicobacter. 2012; 17:374–381.10. Murakami K, Furuta T, Ando T, et al. Multi-center randomized controlled study to establish the standard third-line regimen for Helicobacter pylori eradication in Japan. J Gastroenterol. 2013; 48:1128–1135.11. Tai WC, Lee CH, Chiou SS, et al. The clinical and bacteriological factors for optimal levofloxacin-containing triple therapy in second-line Helicobacter pylori eradication. PLoS One. 2014; 9:e105822.12. Asaka M, Kato M, Takahashi S, et al. Guidelines for the management of Helicobacter pylori infection in Japan:2009 revised edition. Helicobacter. 2010; 15:1–20.13. Hwang TJ, Kim N, Kim HB, et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J Clin Gastroenterol. 2010; 44:536–543.14. Chuah SK, Tsay FW, Hsu PI, Wu DC. A new look at anti-Helicobacter pylori therapy. World J Gastroenterol. 2011; 17:3971–3975.15. Gao W, Cheng H, Hu F, et al. The evolution of Helicobacter pylori antibiotics resistance over 10 years in Beijing, China. Helicobacter. 2010; 15:460–466.16. Kostamo P, Veijola L, Oksanen A, Sarna S, Rautelin H. Recent trends in primary antimicrobial resistance of Helicobacter pylori in Finland. Int J Antimicrob Agents. 2011; 37:22–25.17. Fock KM, Katelaris P, Sugano K, et al. Second Asia-Pacific consensus guidelines for Helicobacter pylori infection. J Gastroenterol Hepatol. 2009; 24:1587–1600.18. Chuah SK, Hsu PI, Chang KC, et al. Randomized comparison of two non-bismuth-containing second-line rescue therapies for Helicobacter pylori. Helicobacter. 2012; 17:216–223.19. Kim JY, Kim NY, Kim SJ, et al. Regional difference of antibiotic resistance of Helicobacter pylori strains in Korea. Korean J Gastroenterol. 2011; 57:221–229.20. Gisbert JP, Romano M, Gravina AG, et al. Helicobacter pylori second-line rescue therapy with levofloxacin- and bismuth-containing quadruple therapy, after failure of standard triple or non-bismuth quadruple treatments. Aliment Pharmacol Ther. 2015; 41:768–775.21. Jeong MH, Chung JW, Lee SJ, et al. Comparison of rifabutin- and levofloxacin-based third-line rescue therapies for Helicobacter pylori. Korean J Gastroenterol. 2012; 59:401–406.22. Zullo A, Hassan C, De Francesco V, et al. A third-line levofloxacin-based rescue therapy for Helicobacter pylori eradication. Dig Liver Dis. 2003; 35:232–236.23. Gisbert JP. "Rescue" regimens after Helicobacter pylori treatment failure. World J Gastroenterol. 2008; 14:5385–5402.24. Li Y, Huang X, Yao L, Shi R, Zhang G. Advantages of Moxifloxacin and Levofloxacin-based triple therapy for second-line treatments of persistent Helicobacter pylori infection: a meta analysis. Wien Klin Wochenschr. 2010; 122:413–422.25. Hirata Y, Ohmae T, Yanai A, et al. Sitafloxacin resistance in Helicobacter pylori isolates and sitafloxacin-based triple therapy as a third-line regimen in Japan. Int J Antimicrob Agents. 2012; 39:352–355.26. Tai WC, Chiu CH, Liang CM, et al. Ten-day versus 14-day levofloxacin-containing triple therapy for second-line anti-Helicobacter pylori eradication in Taiwan. Gastroenterol Res Pract. 2013; 2013:932478.27. Gisbert JP, Romano M, Molina-Infante J, et al. Two-week, highdose proton pump inhibitor, moxifloxacin triple Helicobacter pylori therapy after failure of standard triple or non-bismuth quadruple treatments. Dig Liver Dis. 2015; 47:108–113.28. Kim JM, Kim JS, Kim N, Jung HC, Song IS. Distribution of fluoroquinolone MICs in Helicobacter pylori strains from Korean patients. J Antimicrob Chemother. 2005; 56:965–967.29. Kim JM. Antibiotic resistance of Helicobacter pylori isolated from Korean patients. Korean J Gastroenterol. 2006; 47:337–349.30. Kang MS, Park DI, Yun JW, et al. Levofloxacin-azithromycin combined triple therapy for Helicobacter pylori eradication. Korean J Gastroenterol. 2006; 47:30–36.31. Lee JH, Hong SP, Kwon CI, et al. The efficacy of levofloxacin based triple therapy for Helicobacter pylori eradication. Korean J Gastroenterol. 2006; 48:19–24.32. Jung HS, Shim KN, Baik SJ, et al. Efficacy of levofloxacin-based triple therapy as second-line Helicobacter pylori eradication. Korean J Gastroenterol. 2008; 51:285–290.33. Gatta L, Zullo A, Perna F, et al. A 10-day levofloxacin-based triple therapy in patients who have failed two eradication courses. Aliment Pharmacol Ther. 2005; 22:45–49.
Article34. Gisbert JP, Morena F. Systematic review and metaanalysis: levofloxacin-based rescue regimens after Helicobacter pylori treatment failure. Aliment Pharmacol Ther. 2006; 23:35–44.35. Gisbert JP, Castro-Fernández M, Bermejo F, et al. Third-line rescue therapy with levofloxacin after two H. pylori treatment failures. Am J Gastroenterol. 2006; 101:243–247.36. Gisbert JP, Gisbert JL, Marcos S, Moreno-Otero R, Pajares JM. Third-line rescue therapy with levofloxacin is more effective than rifabutin rescue regimen after two Helicobacter pylori treatment failures. Aliment Pharmacol Ther. 2006; 24:1469–1474.37. Gisbert JP, Pérez-Aisa A, Bermejo F, et al. Second-line therapy with levofloxacin after failure of treatment to eradicate Helicobacter pylori infection: time trends in a Spanish Multicenter Study of 1000 patients. J Clin Gastroenterol. 2013; 47:130–135.38. Chuah SK, Tai WC, Lee CH, Liang CM, Hu TH. Quinolone-containing therapies in the eradication of Helicobacter pylori. Biomed Res Int. 2014; 2014:151543.39. Robicsek A, Jacoby GA, Hooper DC. The worldwide emergence of plasmid-mediated quinolone resistance. Lancet Infect Dis. 2006; 6:629–640.
Article40. Hung KH, Sheu BS, Chang WL, Wu HM, Liu CC, Wu JJ. Prevalence of primary fluoroquinolone resistance among clinical isolates of Helicobacter pylori at a University Hospital in Southern Taiwan. Helicobacter. 2009; 14:61–65.41. Su P, Li Y, Li H, et al. Antibiotic resistance of Helicobacter pylori isolated in the Southeast Coastal Region of China. Helicobacter. 2013; 18:274–279.42. Devasia RA, Blackman A, Gebretsadik T, et al. Fluoroquinolone resistance in Mycobacterium tuberculosis: the effect of duration and timing of fluoroquinolone exposure. Am J Respir Crit Care Med. 2009; 180:365–370.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Efficacy of Levofloxacin Based Triple Therapy for Helicobacter pylori Eradication
- Approach to Patients with Consecutive Helicobacter pylori Eradication Failure
- Recent Update on Third-line Helicobacter pylori Eradication
- Rifaximin Plus Levofloxacin-Based Rescue Regimen for the Eradication of Helicobacter pylori
- Comparison of Rifabutin- and Levofloxacin-based Third-line Rescue Therapies for Helicobacter pylori
