A Case of the Low-Grade, Non-Intestinal type Sinonasal Adenocarcinoma of Nasal Septum
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Daegu Fatima Hospital, Daegu, Korea. teilor@fatima.or.kr
- KMID: 2379792
- DOI: http://doi.org/10.18787/jr.2017.24.1.56
Abstract
- Adenocarcinomas of the sinonasal tract are relatively rare. Such tumors are divided into salivary and nonsalivary types as classified by the World Health Organization. Nonsalivary sinonasal adenocarcinomas are further classified as intestinal (ITAC) and non-intestinal (non-ITAC), which can be separated even further into high-grade and low-grade. Low grade non-ITACs are more uncommon than ITACs. In this study, we present a case of low-grade non-ITAC in a 61-year-old woman who was successfully treated with wide excision without radiotherapy, and we also provide a review of the literature.
Keyword
MeSH Terms
Figure
-

Fig. 1. Endoscopic finding demonstrates polypoid mass between left middle turbinate and septum ( S: septum, M: middle turbinate, arrow: mass).
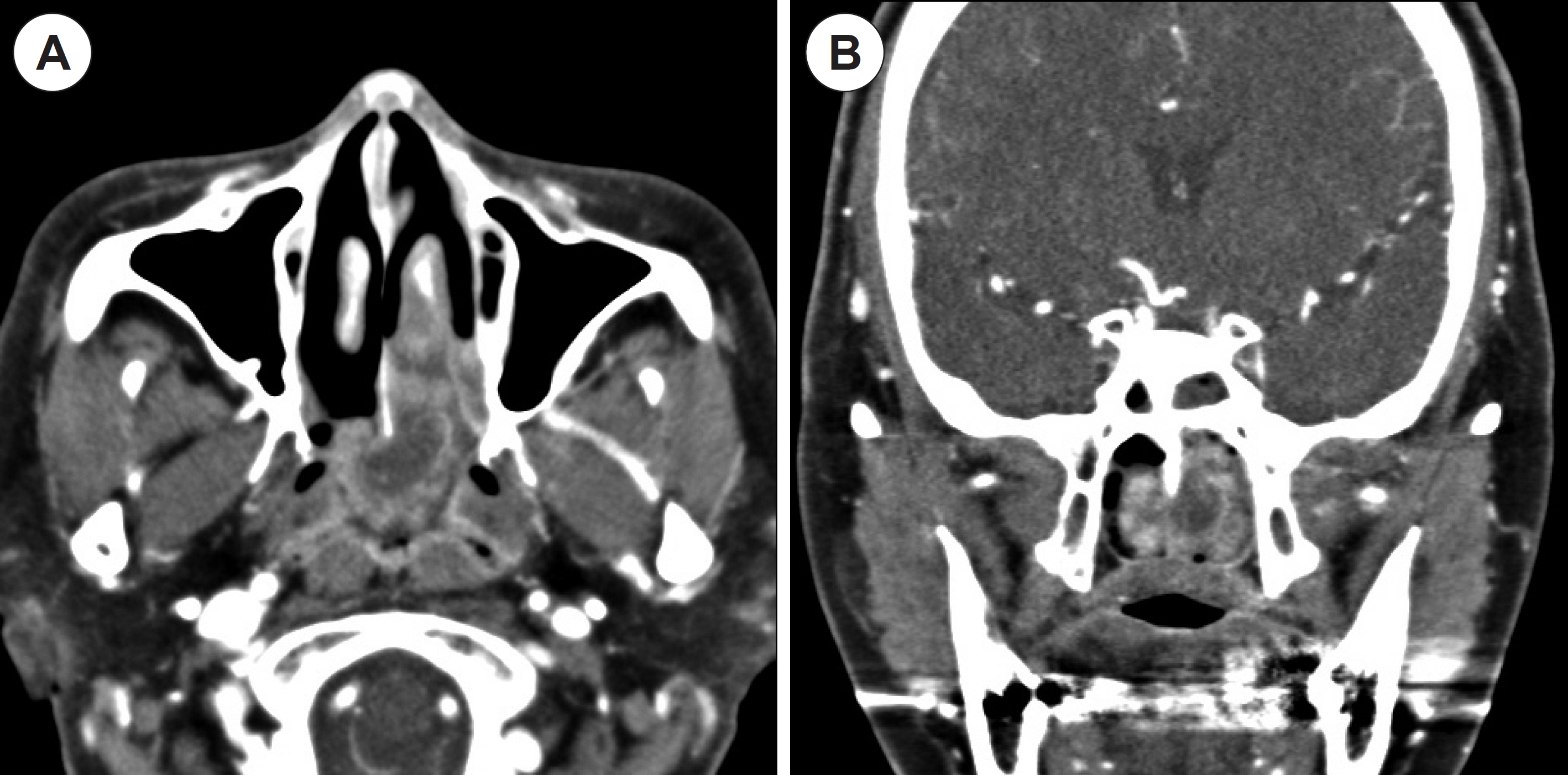
Fig. 2. Contrast-enhanced comput-ed tomography scans show heterogeneously enhancing soft tissue mass occupying both nasal cavities and nasopharynx. Tumor invasion into nasal septum and nasopharynx is suspicious, and soft tissue density in the left sphenoid sinus is observed. ( A) Axial, ( B) Coronal.
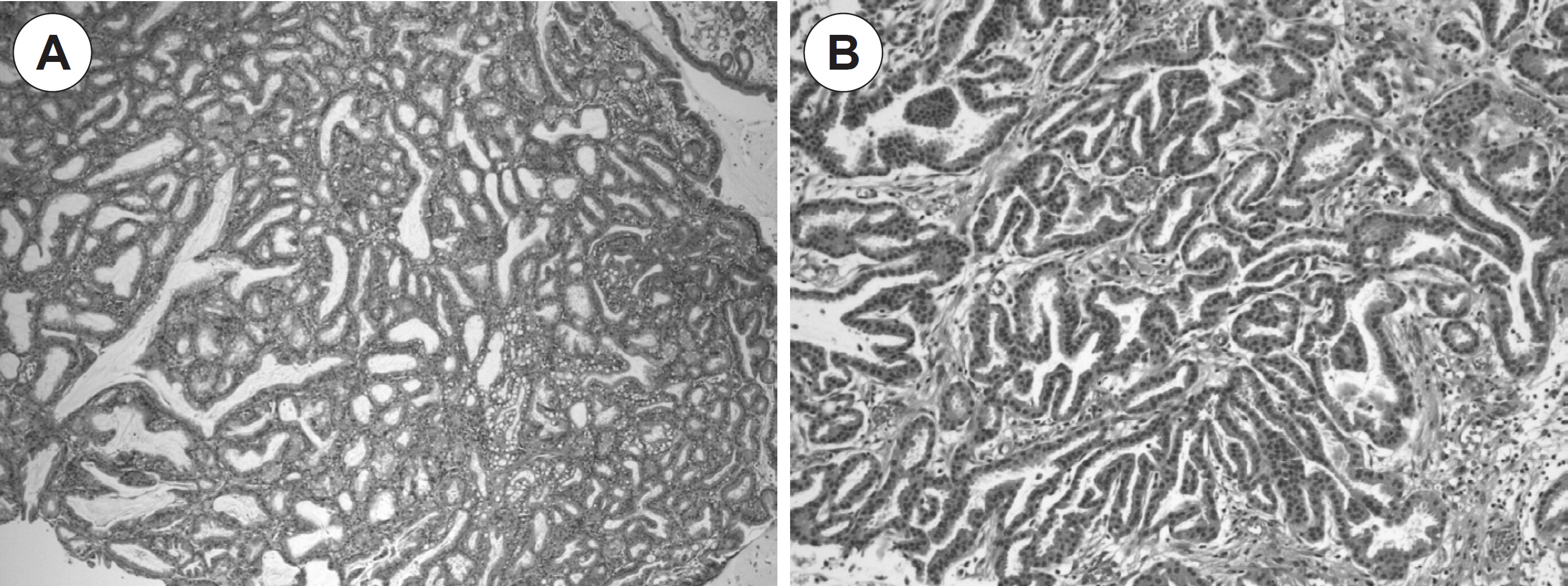
Fig. 3. ( A) Complex glandular growth pattern lacking an intervening fibro-vascular stroma demonstrated by hematoxylin and erosion ( H&E) stain-ing (×40). ( B) Single layer of noncil-liated columnar cells with uniform, round nuclei identified by H&E stain-ing (×100).
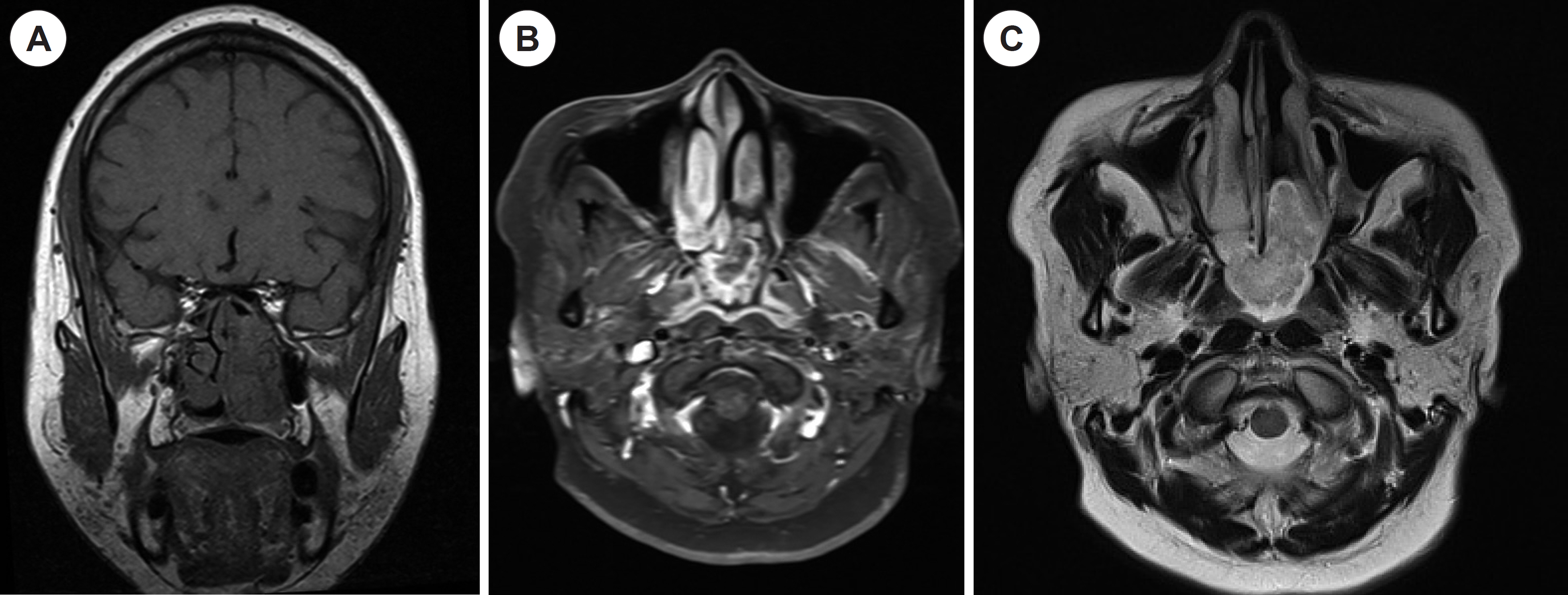
Fig. 4. ( A) Coronal T1 weighted magnetic resonance imaging ( MRI) shows the low signal intensity mass in the left nasal cavity. ( B) Axial Gadolinium-enhanced T1 weighted MRI demonstrates heterogeneously enhancing mass in the both nasal cavities and nasopharynx without invasion of nasal septum and nasopharynx. ( C) Axial T2 weighted MRI reveals the high signal intensity mass, too.
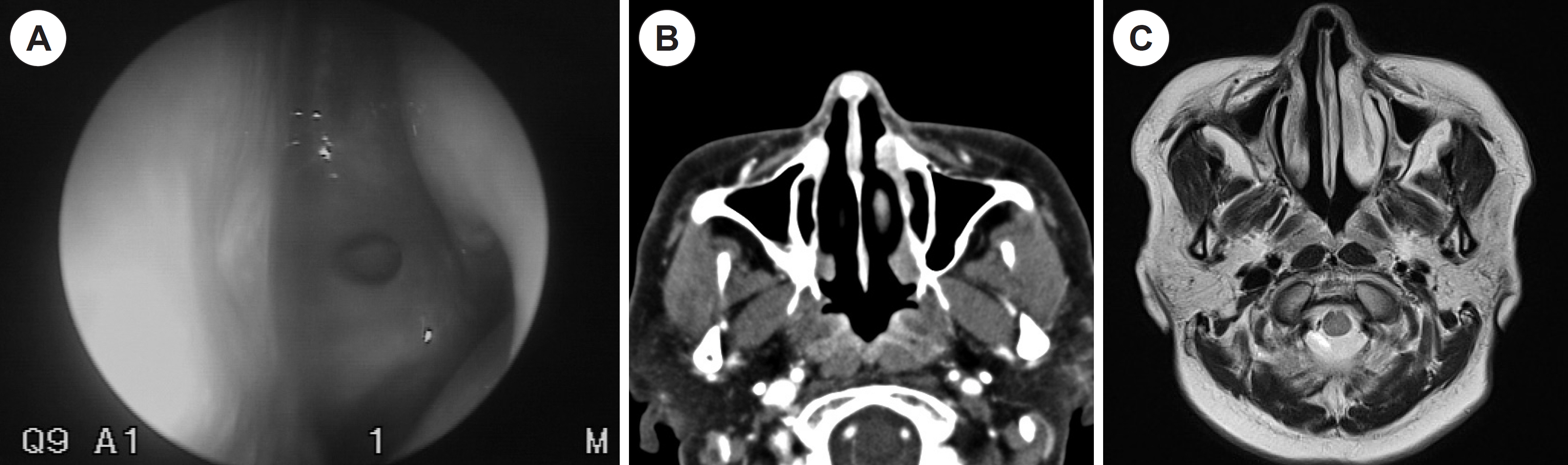
Fig. 5. ( A) Postoperative endoscopic finding, ( B) CT, and ( C) T2 weighted MRI show no evidence of recurrence ( S: septum, O: sphenoid ostium, T: superior turbinate).
Reference
-
1). Blumberg JM, Escobar-Stein J, Vining EM, Prasad ML. Low-Grade, Nonintestinal Nonsalivary Sinonasal Adenocarcinoma Associated With an Exophytic Schneiderian Papilloma: A Case Report. Int J Surg Pathol. 2015; 23:662–6.2). Bhayani MK, Yilmaz T, Sweeney A, Calzada G, Roberts DB, Levine NB, et al. Sinonasal adenocarcinoma: a 16-year experience at a sin-gle institution. Head Neck. 2014; 36:1490–6.
Article3). Lund VJ, Chisholm EJ, Takes RP, Suarez C, Mendenhall WM, Rinal-do A, et al. Evidence for treatment strategies in sinonasal adenocarcinoma. Head Neck. 2012; 34:1168–78.
Article4). Chan Goo L, Young Joo P, Susie C, Jae Yong L. A Case of Papillary Intestinal Type Sinonasal Adenocarcinoma of the nasal cavity. Korean J Otorhinolaryngol-Head Neck Surg. 2013; 56:310–3.
Article5). Franchi A, Santucci M, Wenig BM. Adenocarcinoma. Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and Genet-ics of Head and Neck Tumours. World Health Organization classifi-cation of tumours. 9th ed.Lyon, France: IARC Press;2005. p. 20–3.6). Leivo I. Sinonasal Adenocarcinoma: Update on Classification, Im-munophenotype and Molecular Features. Head Neck Pathol. 2016; 10:68–74.
Article7). Bhaijee F, Carron J, Bell D. Low-grade nonintestinal sinonasal adenocarcinoma: a diagnosis of exclusion. Ann Diagn Pathol. 2011; 15:181–4.
Article8). Meccariello G, Deganello A, Choussy O, Gallo O, Vitali D, De Rau-court D, et al. Endoscopic nasal versus open approach for the management of sinonasal adenocarcinoma: A pooled-analysis of 1826 patients. Head Neck. 2016; 38(Suppl 1):E2267–74.
Article9). Lund VJ, Wei WI. Endoscopic surgery for malignant sinonasal tumours: an eighteen year experience. Rhinology. 2015; 53:204–11.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-Salivary Type Adenocarcinoma of the Sinonasal Tract A case report with low and high grade histologies
- Sinonasal intestinal-type adenocarcinoma in the frontal sinus
- A Case of Papillary Intestinal Type Sinonasal Adenocarcinoma of the Nasal Cavity
- Respiratory Epithelial Adenomatoid Hamartoma Originating from Nasal Septum
- A Case of Sarcoidosis of the Nasal Septum
