Respiratory Epithelial Adenomatoid Hamartoma Originating from Nasal Septum
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, Korea. lhman@korea.ac.kr
Abstract
- Respiratory epithelial adenomatoid hamartoma (REAH) is a rare benign lesion in nasal cavity. We report two cases of REAH of the nasal cavity arising from nasal septum. The etiology of REAH is unknown although inflammation may induce gland proliferation observed in hamartomas. One of our cases was associated with nasal polyposis. REAH is a self-limiting disease, so it is important to differentiate REAH from other pathologic process, including inverted papilloma and low-grade adenocarcinoma. The treatment of choice is complete excision through a conservative approach.
MeSH Terms
Figure
-
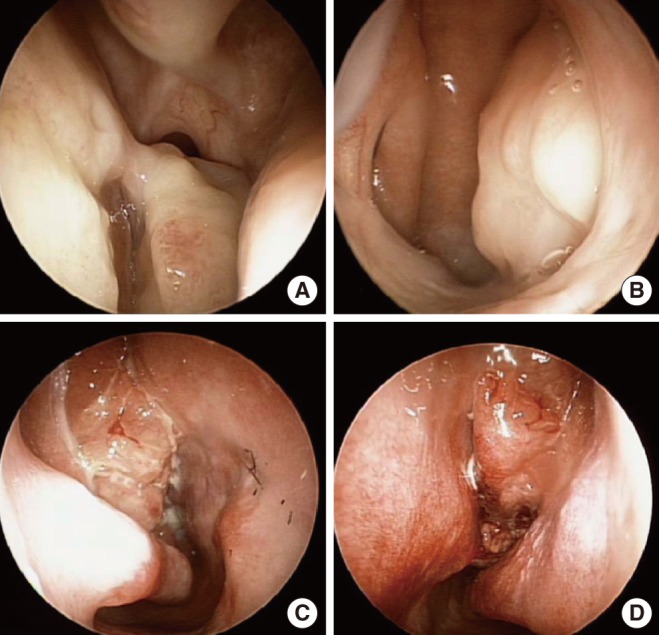
Fig. 1 Nasal endoscopy details of case 1 (A, B) and case 2 (C, D). (A, B) Nasal endoscopic finding revealed a smooth mucosa covered, polypoid mass on the posterior aspect of nasal septum in the left nasal cavity. It was originated from posterior part of septum. The mass extended to right side through the nasopharynx. (C, D) Nasal endoscopy shows bilateral nasal polyposis in middle meatus.
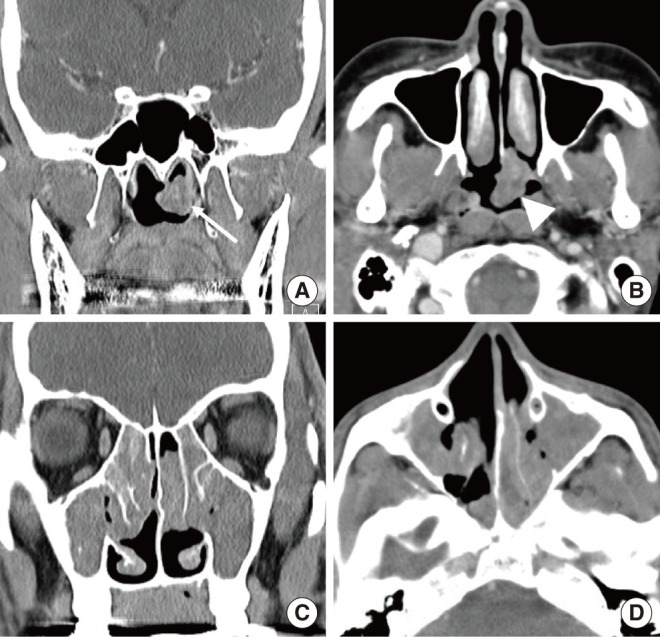
Fig. 2 Computed tomography (CT) details of case 1 (A, B) and case 2 (C, D). (A) CT scan of paranasal sinuses coronal view shows left nasophryngeal mass (white arrow). (B) Axial view reveals the mass is attached to posterior aspect of nasal septum (white arrow head). (C) Coronal view and (D) axial view of CT scan of paranasal sinus showed soft tissue density in maxillary and ethmoid sinus and both nasal cavity.
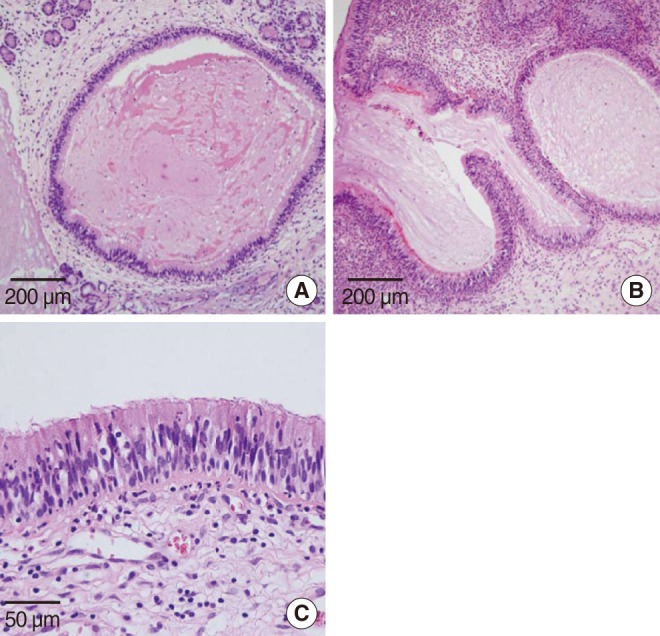
Fig. 3 Microscopy details of case 1 (A) and case 2 (B, C). (A) Proliferated gland was lined by ciliated respiratory epithelium. No atypical cell was seen and there was no evidence of metaplasia (H&E, ×100). (B) Photomicroscopic finding shows elongated invaginations into the lamina propria. Glandular proliferation originating from the invaginating surface epithelium was seen (H&E, ×100). (C) The lining of gland was ciliated respiratory epithelium (H&E, ×400).
Reference
-
1. Delbrouck C, Fernandez Aguilar S, Choufani G, Hassid S. Respiratory epithelial adenomatoid hamartoma associated with nasal polyposis. Am J Otolaryngol. 2004; Jul-Aug. 25(4):282–284. PMID: 15239039.
Article2. Endo R, Matsuda H, Takahashi M, Hara M, Inaba H, Tsukuda M. Respiratory epithelial adenomatoid hamartoma in the nasal cavity. Acta Otolaryngol. 2002; 6. 122(4):398–400. PMID: 12125996.
Article3. Birt BD, Knight-Jones EB. Respiratory distress due to nasopharyngeal hamartoma. Br Med J. 1969; 8. 3(5665):281–282. PMID: 5800369.
Article4. Wenig BM, Heffner DK. Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: a clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol. 1995; 8. 104(8):639–645. PMID: 7639474.
Article5. Himi Y, Yoshizaki T, Sato K, Furukawa M. Respiratory epithelial adenomatoid hamartoma of the maxillary sinus. J Laryngol Otol. 2002; 4. 116(4):317–318. PMID: 11945202.
Article6. Metselaar RM, Stel HV, van der Baan S. Respiratory epithelial adenomatoid hamartoma in the nasopharynx. J Laryngol Otol. 2005; 6. 119(6):476–478. PMID: 15992477.
Article7. Kessler HP, Unterman B. Respiratory epithelial adenomatoid hamartoma of the maxillary sinus presenting as a periapical radiolucency: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 5. 97(5):607–612. PMID: 15153874.
Article8. Liang J, O'Malley BW Jr, Feldman M, Newman JG. A case of respiratory epithelial adenomatoid hamartoma. Am J Otolaryngol. 2007; Jul-Aug. 28(4):277–279. PMID: 17606048.
Article9. Ozolek JA, Hunt JL. Tumor suppressor gene alterations in respiratory epithelial adenomatoid hamartoma (REAH): comparison to sinonasal adenocarcinoma and inflamed sinonasal mucosa. Am J Surg Pathol. 2006; 12. 30(12):1576–1580. PMID: 17122514.10. Kaneko C, Inokuchi A, Kimitsuki T, Kumamoto Y, Shinokuma A, Natori Y, et al. Huge hamartoma with inverted papilloma in the nasal cavity. Eur Arch Otorhinolaryngol. 1999; 256(Suppl 1):S33–S37. PMID: 10337524.
Article11. Lima NB, Jankowski R, Georgel T, Grignon B, Guillemin F, Vignaud JM. Respiratory adenomatoid hamartoma must be suspected on CT-scan enlargement of the olfactory clefts. Rhinology. 2006; 12. 44(4):264–269. PMID: 17216743.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Respiratory Epithelial Adenomatoid Hamartoma in Nasal Cavity
- A Case of Chondro-Osseous Respiratory Epithelial Adenomatoid Hamartoma Originated from Nasal Cavity
- A Case of Adenomatoid Hamartoma Originated from Nasal Cavity
- Respiratory Epithelial Adenomatoid Hamartoma at an Unusual Location: A Case Report and Literature Review
- A Case of Inverted Papilloma Originating from Posterior Nasal Septum
