Korean J Gastroenterol.
2015 Aug;66(2):122-126. 10.4166/kjg.2015.66.2.122.
Complete Tumor Resection for a Hepatocellular Carcinoma Secreting Parathyroid Hormone-related Peptide
- Affiliations
-
- 1Department of Internal Medicine, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea. yhkumd@gmail.com
- 2Department of Surgery, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea.
- KMID: 2373325
- DOI: http://doi.org/10.4166/kjg.2015.66.2.122
Abstract
- Hepatocellular carcinoma (HCC) is the fifth most common cancer in Korea. Diverse paraneoplastic syndromes can occur in patients with HCC, but parathyroid hormone-related peptide (PTH-rP)-induced hypercalcemia is uncommon. Hypercalcemia due to PTH or particularly PTH-rP-secreting HCC is associated with poor outcomes. We report a 71-year-old man who presented with symptoms of vague abdominal discomfort, somnolence, lethargy, nausea, vomiting, and weight loss. Imaging studies revealed a large HCC without metastasis. The laboratory findings showed elevated serum calcium level, low intact parathyroid hormone (iPTH) level and elevated PTH-rP level. These results led to a diagnosis of a PTH-rP-secreting HCC and paraneoplastic hypercalcemia. After emergency management of the hypercalcemia, the patient underwent an extended right hemihepatectomy with cholecystectomy. One year after the surgery, he is alive with normal calcium, PTH-rP, and iPTH levels. This case demonstrates that the rare phenomenon of life-threatening hypercalcemia caused by HCC should not be overlooked. These symptoms offer a good opportunity to diagnose HCC early. Radical tumor resection makes it possible to cure patients with PTH-rP-secreting HCC.
MeSH Terms
Figure
-
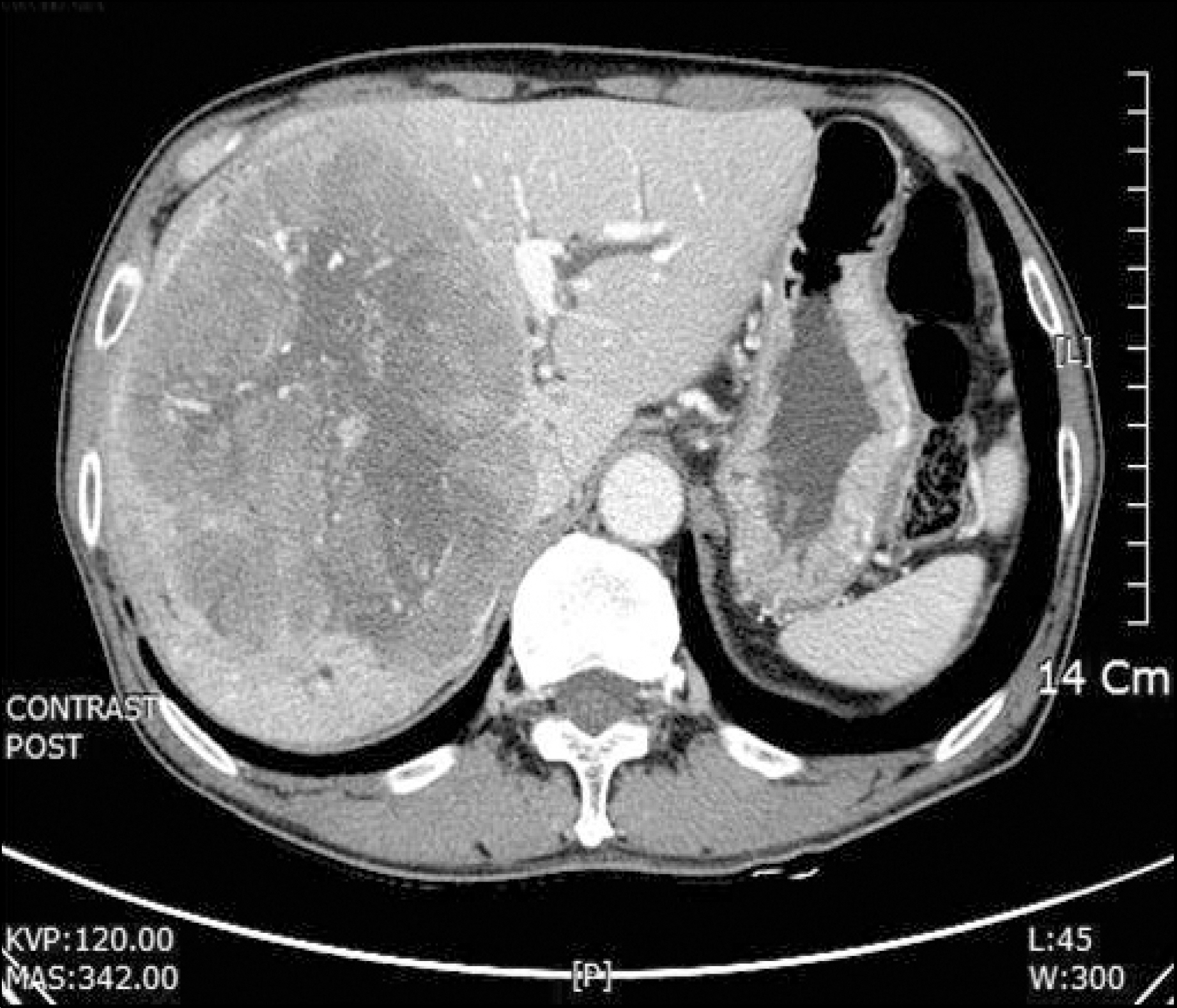
Fig. 1. Hepatocellular carcinoma at the time of diagnosis. A 13-cm tumor is visualized in the right hepatic lobe.
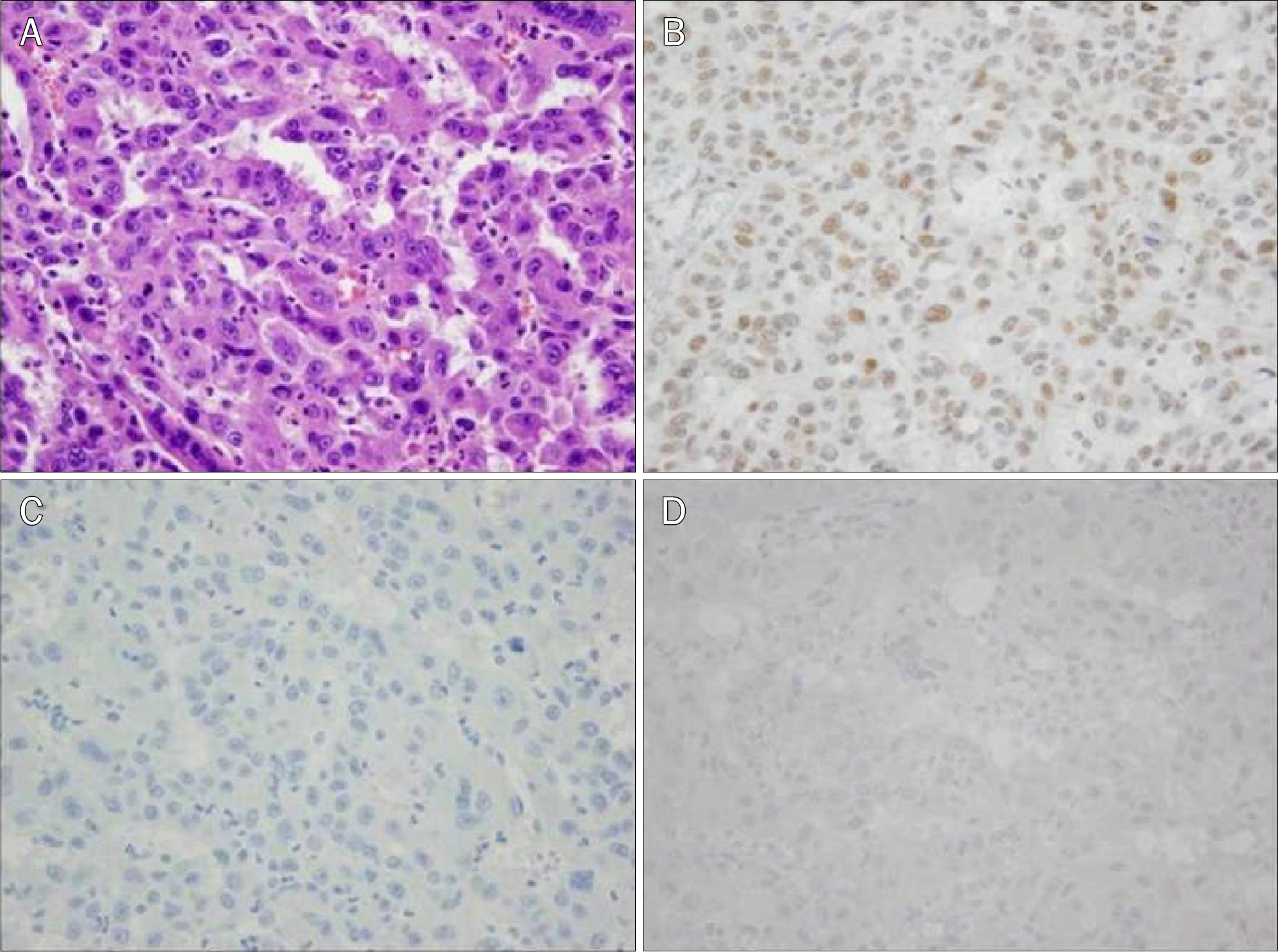
Fig. 2. Immunohistochemistry of the tumor specimen. (A) Microscopically tumor cells show trabecular growth patterns separated by sinusoids (H&E, ×400). (B) Positive staining for glypican-3 (×400). (C) Negative staining for CK19 (×400). (D) Negative staining for parathyroid hormone (×400).
Reference
-
References
1. Stewart AF, Horst R, Deftos LJ, Cadman EC, Lang R, Broadus AE. Biochemical evaluation of patients with cancer-associated hypercalcemia: evidence for humoral and nonhumoral groups. N Engl J Med. 1980; 303:1377–1383.2. Huh UY, Kim JH, Kim BH, et al. The incidence and clinical significance of paraneoplastic syndromes in patients with hepatocellular carcinoma. Korean J Hepatol. 2005; 11:275–283.3. Chu CW, Hwang SJ, Luo JC, et al. Manifestations of hyper-cholesterolaemia, hypoglycaemia, erythrocytosis and hyper-calcaemia in patients with hepatocellular carcinoma: report of two cases. J Gastroenterol Hepatol. 1999; 14:807–810.
Article4. Luo JC, Hwang SJ, Wu JC, et al. Clinical characteristics and prognosis of hepatocellular carcinoma patients with paraneoplastic syndromes. Hepatogastroenterology. 2002; 49:1315–1319.5. Oldenburg WA, van Heerden JA, Sizemore GW, Abboud CF, Sheedy PF 2nd. Hypercalcemia and primary hepatic tumors. Arch Surg. 1982; 117:1363–1366.
Article6. Chang PE, Ong WC, Lui HF, Tan CK. Epidemiology and prognosis of paraneoplastic syndromes in hepatocellular carcinoma. ISRN Oncol. 2013. DOI: doi:10.1155/2013/684026.
Article7. Lumachi F, Brunello A, Roma A, Basso U. Medical treatment of malignancy-associated hypercalcemia. Curr Med Chem. 2008; 15:415–421.
Article8. Ralston SH, Gallacher SJ, Patel U, Campbell J, Boyle IT. Cancerassociated hypercalcemia: morbidity and mortality. Clinical experience in 126 treated patients. Ann Intern Med. 1990; 112:499–504.9. Ghobrial MW, George J, Mannam S, Henien SR. Severe hypercalcemia as an initial presenting manifestation of hepatocellular carcinoma. Can J Gastroenterol. 2002; 16:607–609.
Article10. Mahoney EJ, Monchik JM, Donatini G, De Lellis R. Life-threat-ening hypercalcemia from a hepatocellular carcinoma secreting intact parathyroid hormone: localization by sestamibi single-photon emission computed tomographic imaging. Endocr Pract. 2006; 12:302–306.
Article11. Lee MH, Son JH, Jang WY, et al. A case of hepatocellular carcinoma with hypercholesterolemia and hypercalcemia as paraneoplastic syndrome. Korean J Gastroenterol. 1999; 34:271–276.12. Kim JH, Kim BH, Lee DH, et al. A case of hepatocellular carcinoma presenting with four paraneoplastic syndromes such as hypercholesterolemia, hypoglycemia, hypercalcemia, and erythrocytosis. Korean J Gastroenterol. 2003; 41:316–320.13. Lee D, Kim IH, Kim SH, et al. A case of sclerosing hepatocellular carcinoma with hypercalcemia treated with transcatheter arterial chemoembolization. Korean J Med. 2000; 59:104–108.14. Yoon SY, Lee CR, Lee JH, Choi SJ, Son SP. A case of humoral hypercalcemia of malignancy associated with hepatoma: a case in which both PTHrP and 1,25 (OH) 2D were elevated. J Korean Soc Endocrinol. 1999; 14:197–202.15. Berenson JR. Treatment of hypercalcemia of malignancy with bisphosphonates. Semin Oncol. 2002; 29(6 Suppl 21):12–18.
Article16. Bilezikian JP, Singer FR. Acute management of hypercalcemia due to parathyroid hormone and parathyroid hormone-related protein. Bilezikian JP, Marcus R, Levine MA, editors. The Parathyroids: basic and clinical concepts. New York: Raven Press;1994. p. 359–372.17. Stewart AF. Clinical practice. Hypercalcemia associated with cancer. N Engl J Med. 2005; 352:373–379.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonfunctional Parathyroid Carcinoma: A Case Report
- Parathyroid carcinoma with lung metastasis in a thirteen-year-old girl
- A Case of Hepatocellular Carcinoma with Hypercholesterolemia and Hypercalcemia as Paraneoplastic Syndrome
- Hypercalcemia as Initial Presentation of Metastatic Adenocarcinoma of Gastric Origin: A Case Report and Review of the Literature
- A case of hepatocellular carcinoma combined with solitary parathyroid metastasis
