Benign Fibrous Histiocytoma with Cystic Change of the Femur: a Case Report
- Affiliations
-
- 1Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. sgsgmoon@gmail.com
- KMID: 2366410
- DOI: http://doi.org/10.13104/imri.2016.20.4.264
Abstract
- Benign fibrous histiocytoma (BFH) is a rare benign primary skeletal tumor that occurs commonly in the long bones, spine and pelvis. BFH constitutes a diagnostic challenge because it shares clinical background, radiological characteristics, and histological features with other fibrous lesions such as non-ossifying fibroma, giant cell tumor. We present a case of BFH with cystic change that occurred in the distal femur. We did not identify any case of BFH with cystic change involving the majority of the lesion that occurred in the metaepiphysis of the long bone.
Figure
-

Fig. 1 Plain radiograph demonstrated an eccentrically located, and radiolucent lesion in the metaepiphysis of the distal femur. The lateral cortex was thinned and expansile. The osteolytic lesion had a partially marginal sclerosis along the medial border without intralesional matrix mineralization.
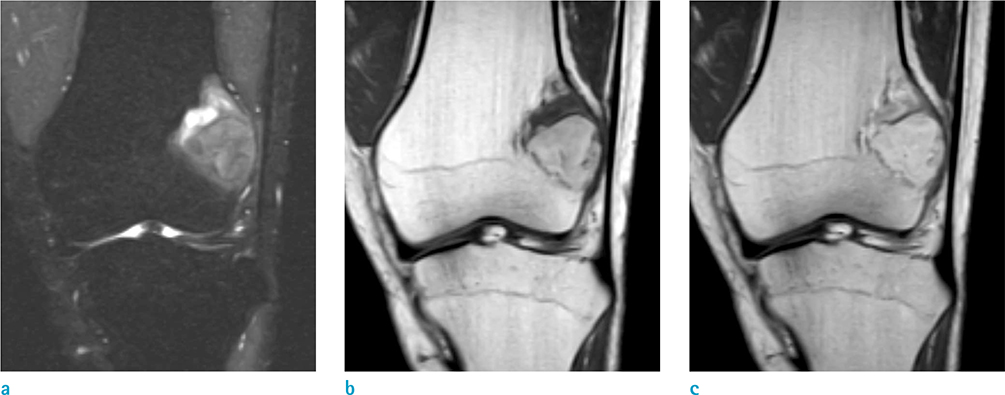
Fig. 2 Magnetic resonance imaging of BFH of the distal femur. (a) Coronal proton density-weighted image with fat suppression demonstrated an expansile heterogeneous mass in lateral aspect of the metaphysis of the distal femur extending to the epiphysis. The majority of the mass consists of intermediate hyperintense lesion with curvilinear, hyperintense component superiorly. (b) On T1-weighted coronal image, the majority of the mass appeared hyperintense, but the curvilinear part revealed hypointense superiorly. (c) On postcontrast image, the superior part of the mass showed strong enhancement meaning solid component, and the majority part of the mass showed no enhancement suggesting hemorrhagic component.

Fig. 3 Bone scan showed an intense radiotracer uptake in left distal femur.
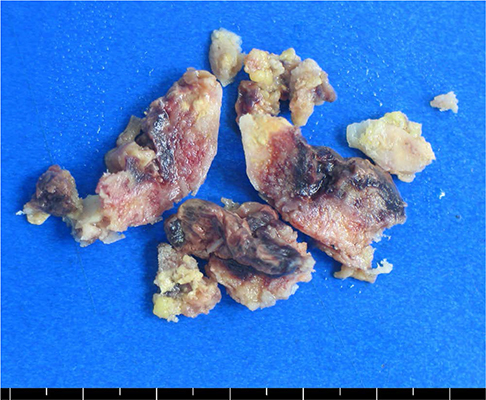
Fig. 4 Surgical specimens revealed several fragments of gray-brown-colored, irregular solid components with overt hemorrhage occupying the majority of the mass.
Reference
-
1. Grohs JG, Nicolakis M, Kainberger F, Lang S, Kotz R. Benign fibrous histiocytoma of bone: a report of ten cases and review of literature. Wien Klin Wochenschr. 2002; 114:56–63.2. Clarke BE, Xipell JM, Thomas DP. Benign fibrous histiocytoma of bone. Am J Surg Pathol. 1985; 9:806–815.3. Bertoni F, Calderoni P, Bacchini P, et al. Benign fibrous histiocytoma of bone. J Bone Joint Surg Am. 1986; 68:1225–1230.4. Matsuno T. Benign fibrous histiocytoma involving the ends of long bone. Skeletal Radiol. 1990; 19:561–566.5. Ceroni D, Dayer R, De Coulon G, Kaelin A. Benign fibrous histiocytoma of bone in a paediatric population: a report of 6 cases. Musculoskelet Surg. 2011; 95:107–114.6. Keskinbora M, Kose O, Karslioglu Y, Demiralp B, Basbozkurt M. Another cystic lesion in the calcaneus: benign fibrous histiocytoma of bone. J Am Podiatr Med Assoc. 2013; 103:141–144.7. Hamada T, Ito H, Araki Y, Fujii K, Inoue M, Ishida O. Benign fibrous histiocytoma of the femur: review of three cases. Skeletal Radiol. 1996; 25:25–29.8. Pattamparambath M, Sathyabhama S, Khatri R, Varma S, Narayanan NM. Benign fibrous histiocytoma of mandible: a case report and updated review. J Clin Diagn Res. 2016; 10:ZD24–ZD26.9. Murphey MD, Nomikos GC, Flemming DJ, Gannon FH, Temple HT, Kransdorf MJ. From the archives of AFIP. Imaging of giant cell tumor and giant cell reparative granuloma of bone: radiologic-pathologic correlation. Radiographics. 2001; 21:1283–1309.10. O'Donnell P, Saifuddin A. The prevalence and diagnostic significance of fluid-fluid levels in focal lesions of bone. Skeletal Radiol. 2004; 33:330–336.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Deep Aneurysmal Benign Fibrous Histiocytoma with Atypical Clinical Features
- Deep Benign Fibrous Histiocytoma Showing Multiple Metastases
- Comments to "Deep Benign Fibrous Histiocytoma Showing Multiple Metastases"
- A Case of Subcutaneous Benign Fibrous Histiocytoma
- A Case of Aneurysmal Benign Fibrous Histiocytoma
