Collision Tumor Composed of Meningioma and Cavernoma
- Affiliations
-
- 1Department of Neurosurgery, Paracelsus Medical University, General Hospital Nuremberg, Nuremberg, Germany. jens.weigel@klinikum-nuernberg.de
- 2Institute of Pathology, Paracelsus Medical University, General Hospital Nuremberg, Nuremberg, Germany.
- KMID: 2365595
- DOI: http://doi.org/10.3340/jkns.2015.0707.011
Abstract
- A true collision tumor is a rare entity composed of two histologically distinct neoplasms coinciding in the same organ. This paper reports a unique case of cerebral collision tumor consisting of two benign components. On the first hand, meningioma which is usually a benign lesion arising from the meningothelial cell in the arachnoidal membrane. On the other, cerebral cavernoma which is a well-circumscribed, benign vascular hamartoma within the brain. To our knowledge, there is no previously documented case of cerebral collision tumor consisting of two benign components. A 56-year-old Caucasian male suffered in 2002 from an atypical meningioma WHO II° located in the left lateral ventricle. Three years after the tumor extirpation, the patient suffered from a hematoma in the fourth ventricle due to a recurrently haemorrhaged cavernoma. In 2008, a recurrence of the tumor in the left lateral ventricle was discovered. Additionally, another tumor located in the quadrigeminal lamina was detected. After surgical resection of the tumor in the left lateral ventricle, the pathological examination confirmed the diagnosis of a collision tumor consisting of components of a meningioma WHO II° and a cavernoma. Postoperatively, no adjuvant treatment was needed and no tumor recurrence is discovered up to the present. A possible explanation for the collision of those two different tumors may be migration of tumor cells mediated by the cerebrospinal fluid. After 5-years of follow-up, there is no sign of any tumor recurrence; therefore, surgical tumor removal without adjuvant therapy seems to be the treatment of choice.
Keyword
MeSH Terms
Figure
-

Fig. 1 Atypical menigeoma (Haematoxylin-Eosin [HE] stain).

Fig. 2 Mib1-stain.

Fig. 3 A : T1-weighted axial MR image after contrast administration showing the tumor before the last operation. B : T2-weighted sagittal MR image showing the tumor before the last operation. MR : magnetic resonance.

Fig. 4 A : T1 weighted axial MR image after contrast administration showing the tumor in the quadrigeminal lamina. B : T1 weighted sagittal MR image after contrast administration showing the tumor in the quadrigeminal lamina. MR : magnetic resonance.
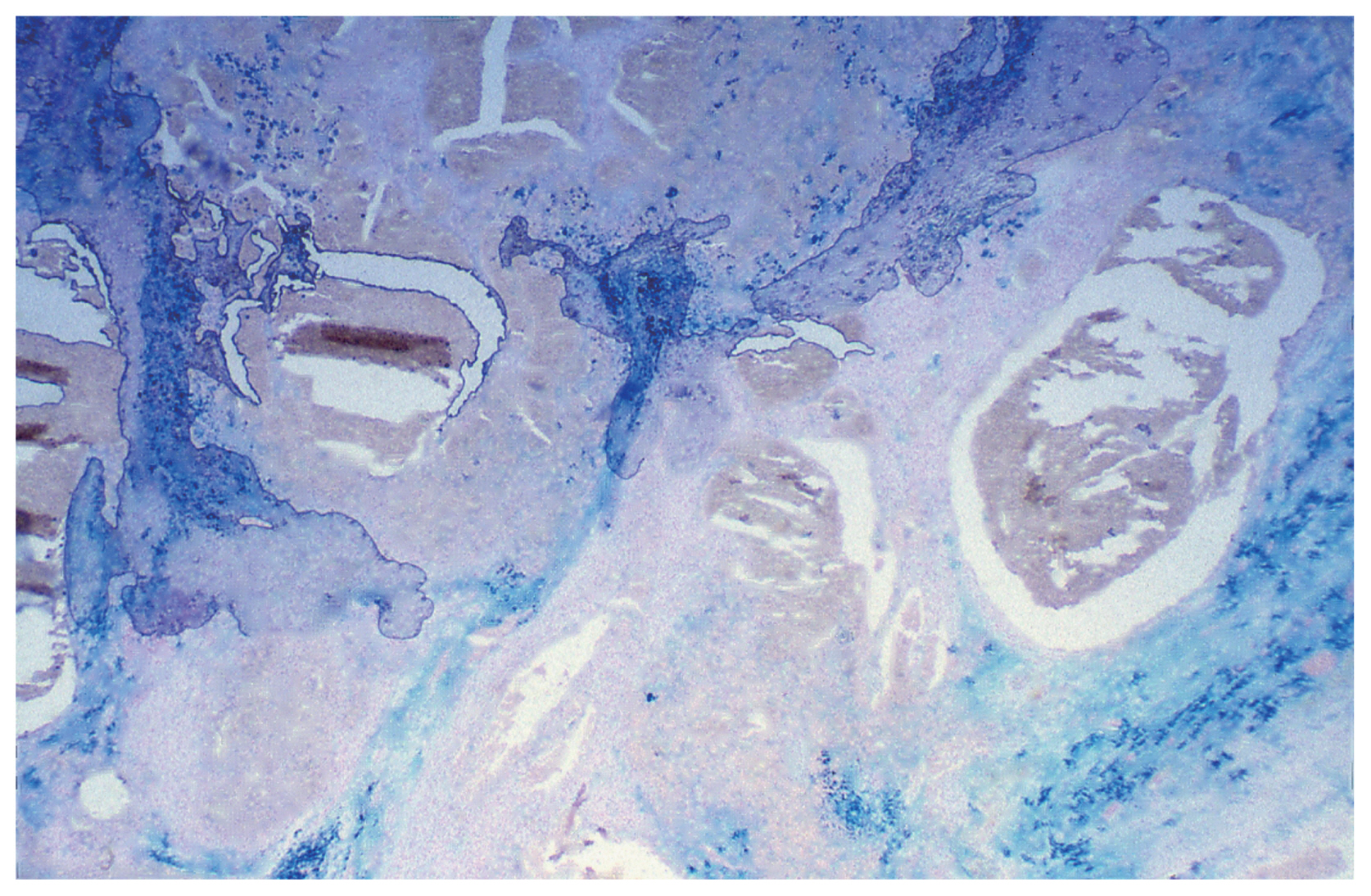
Fig. 5 Cavernoma. EVG stain. EVG : Elastica-van-Gieson.

Fig. 6 EMA stain. EMA : epithelial membrane antigen.

Fig. 7 Collision of Cavernoma and Meningeoma, showing positive staining for EMA and EVG stain. EMA : epithelial membrane antigen, EVG : Elastica-van-Gieson.

Fig. 8 A : T1 weighted axial MR image after contrast administration after tumor extirpation. B : T1 weighted axial MR image after contrast administration, three year follow up. MR : magnetic resonance.
Reference
-
References
1. Cavalcanti DD, Kalani MY, Martirosyan NL, Eales J, Spetzler RF, Preul MC. Cerebral cavernous malformations: from genes to proteins to disease. J Neurosurg. 116:122–132. 2012.
Article2. Dewan S, Alvarez VE, Donahue JE, Cielo D. Intracranial collision metastases of prostate and esophageal carcinoma. J Neurooncol. 95:147–150. 2009.
Article3. Drlicek M1, Aichholzer M, Wurm G, Bodenteich A, Fischer J. Collisiontumour composed of glioblastoma and meningioma-a case report. Pathologe. 25:402–405. 2004.4. Greenberg MS. Handbook of neurosurgery. ed 6. Tampa: Greenberg Graphics, Inc.;2006. p. 426–429. p. 841–843.5. Maier H, Ofner D, Hittmair A, Kitz K, Budka H. Classic, atypical, and anaplastic meningioma: three histopathological subtypes of clinical relevance. J Neurosurg. 77:616–623. 1992.
Article6. Mitsos AP, Konstantinou EA, Fotis TG, Lafazanos SA, Kontogeorgos G, Georgakoulias NV. Sphenoid wing meningioma and glioblastoma multiforme in collision - case report and review of the literature. Neurol Neurochir Pol. 43:479–483. 2009.7. Nestler U, Schmidinger A, Schulz C, Huegens-Penzel M, Gamerdinger UA, Koehler A, et al. Glioblastoma simultaneously present with meningioma--report of three cases. Zentralbl Neurochir. 68:145–150. 2007.
Article8. Palka KT, Lebow RL, Weaver KD, Kressin MK. Intracranial collision metastases of small-cell lung cancer and malignant melanoma. J Clin Oncol. 26:2042–2046. 2008.
Article9. Prayson RA, Chowdhary S, Woodhouse S, Hanson M, Nair S. Collision of a syncytial meningioma and malignant astrocytoma. Ann Diagn Pathol. 6:44–48. 2002.
Article10. Vaquero J, Coca S, Martínez R, Jiménez C. Convexity meningioma and glioblastoma in collision. Surg Neurol. 33:139–141. 1990.
Article11. Willis RA. Structure and growth of tumors. Pathology of tumors. ed 4. London: Butterworth;1967. p. 138.12. Wrobel G, Roerig P, Kokocinski F, Neben K, Hahn M, Reifenberger G, et al. Microarray-based gene expression profiling of benign, atypical and anaplastic meningiomas identifies novel genes associated with meningioma progression. Int J Cancer. 114:249–256. 2005.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Collision Tumor of Meningioma and Anaplastic Astrocytoma
- Collision Tumors in Meningioma:Subtemporal Meningotheliomatous Meningioma and Subtemporal and Infratentorial Psammomatous Meningioma: Case Report
- A Case of Collision Tumor Composed of Dermatofibroma and Ito Nevus
- Collision Tumor of the Liver (Hepatocellular Carcinoma and Undifferentiated Sarcoma)
- Collision Tumor Composed of Papillary Transitional Cell Carcinoma, and Osteosarcoma in Urinary Bladder: A cases report
