Iatrogenic Central Retinal Artery Occlusion Following Retrobulbar Anesthesia for Intraocular Surgery
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@snu.ac.kr
- KMID: 2363767
- DOI: http://doi.org/10.3341/kjo.2015.29.4.233
Abstract
- PURPOSE
To present clinical features of central retinal artery occlusion (CRAO) following retrobulbar anesthesia for intraocular surgery.
METHODS
This observational case series describes 5 consecutive patients with acute CRAO following retrobulbar anesthesia for intraocular surgery. Data collected for this study included subject characteristics, retrobulbar anesthesia technique, treatment type, initial and final best-corrected visual acuity, and other ophthalmologic examinations.
RESULTS
Mean subject age was 67.0 +/- 8.2 years (range, 53 to 72 years). All patients had one or more vascular risk factors (e.g., hypertension, cerebral infarction, carotid artery stenosis) and presented with acute vision loss 1 day after uneventful intraocular surgery (cataract surgery in 2 eyes and vitrectomy in 3 eyes). All 5 patients received retrobulbar anesthesia during surgery, 4 of which involved the use of a sharp needle. No immediate complications were noted during intraocular surgery. Final visual prognosis was poor (from finger count to no light perception) although intraocular thrombolysis was attempted in 3 patients.
CONCLUSIONS
Iatrogenic CRAO is a potential complication of retrobulbar anesthesia for intraocular surgery in elderly patients with vascular risk factors. Unfortunately, this complication can lead to severe vision loss. We conclude that retrobulbar anesthesia for intraocular surgery should be performed with great care and special consideration for elderly patients with vascular risk factors.
MeSH Terms
-
Aged
Anesthesia/*adverse effects/methods
Anesthetics, Local/administration & dosage/*adverse effects
Female
Fluorescein Angiography
Follow-Up Studies
Fundus Oculi
Humans
*Iatrogenic Disease
Male
Middle Aged
Ophthalmologic Surgical Procedures/*adverse effects
Orbit
*Postoperative Complications
Retinal Artery Occlusion/diagnosis/*etiology
Retrospective Studies
Visual Acuity
Anesthetics, Local
Figure
-
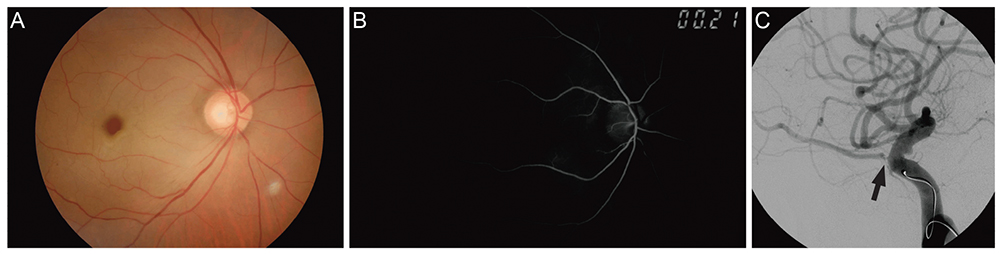
Fig. 1 Images of patient 1 who underwent cataract surgery (phacoemulsification and posterior chamber intraocular lens implant) with retrobulbar anesthesia. (A) Fundus photograph showing a cherry-red spot. (B) Fluorescein angiogram showing decreased choroidal perfusion and delayed filling of the retinal artery and vein. (C) Internal carotid angiogram showing stenosis of the right ophthalmic artery (arrow) and a tortuous proximal ophthalmic artery.
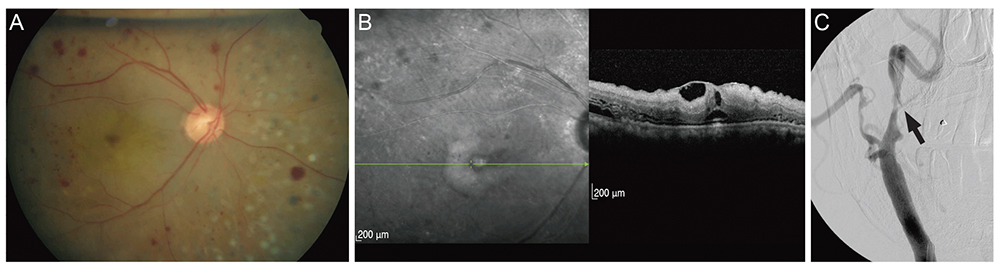
Fig. 2 Images of patient 2 who underwent vitrectomy, endolaser, and intravitreal air injection for proliferative diabetic retinopathy vitreous hemorrhage. (A) Fundus photograph obtained 3 days after intraarterial thrombolysis. A cherry-red spot, retinal edema, and multiple retinal hemorrhages are apparent. (B) Spectral domain optical coherence tomography image obtained 3 days after intra-arterial thrombolysis. Increased reflectivity and inner retinal thickness (including the central macula), along with decreased outer retina reflectivity, are apparent. (C) Internal carotid angiogram showing severe stenosis of the right cervical internal carotid artery (arrow) and the ophthalmic artery.
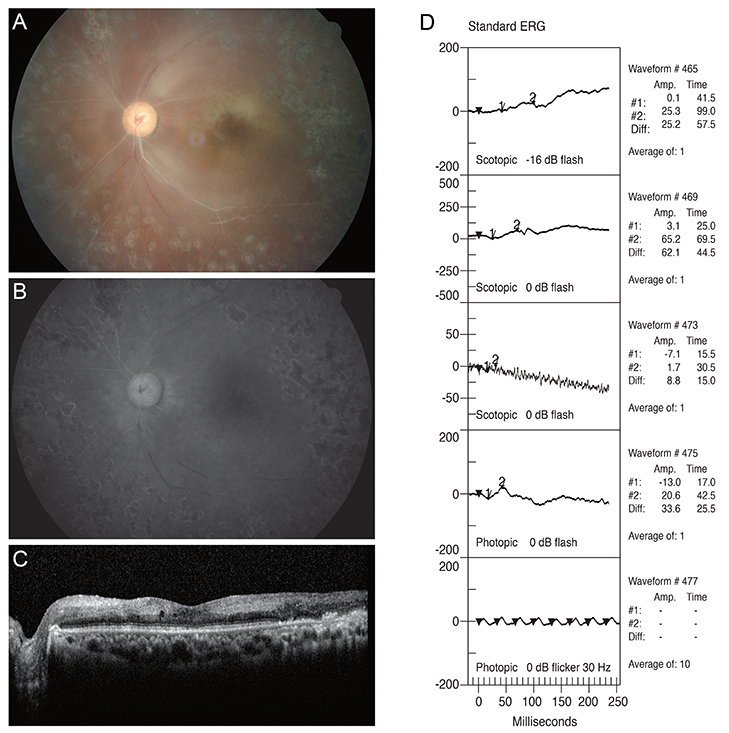
Fig. 3 Images of patient 3, who presented with severe visual decline resulting in no light perception after vitrectomy with retrobulbar anesthesia for proliferative diabetic retinopathy and vitreous hemorrhage. All images were taken 7 days after surgery. (A) A cherry-red spot and severe arterial narrowing and sclerosis are observed in the fundus photograph. (B) Early-phase (2 : 11) fluorescein angiogram showing poor arterial filling. (C) Increased reflectivity and thickness of the inner retina are apparent in spectral domain optical coherence tomography. (D) Standard electroretinogram (ERG) in the left eye showing decreases in both scotopic and photopic wave amplitude.
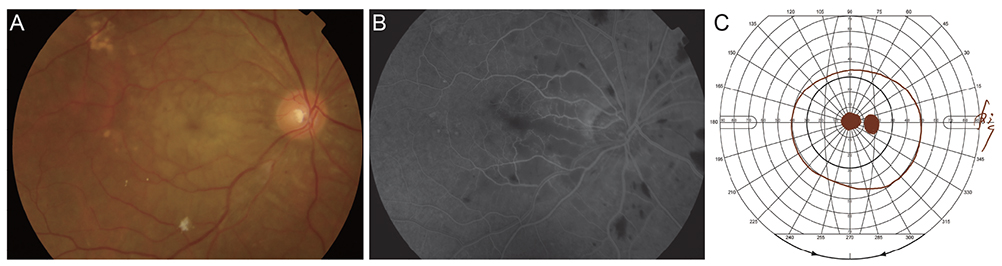
Fig. 4 Images of patient 4, who underwent vitrectomy under retrobulbar anesthesia for treatment of epiretinal membrane. Preoperative best-corrected visual acuity was 20 / 32 in the right eye. One day following surgery, best-corrected visual acuity was at the level of "hand motion" in his right eye. (A) Fundus photograph 1 day after surgery, showing a cherry red spot and marked inner retinal edema in the macula. (B) Early-phase (20 seconds after fluorescein injection) fundus fluorescein angiography 13 days after surgery, showing a mild delay in arteriovenous transit time and multiple patchy capillary nonperfusion in the posterior pole. (C) Goldmann visual field test obtained 5 months after surgery, indicating the presence of a central scotoma.

Fig. 5 Images of patient 5, who underwent cataract surgery (phacoemulsification and posterior chamber intraocular lens implant) under retrobulbar anesthesia and presented with visual decline 1 day after surgery. (A) Fundus photograph 1 day after surgery, showing a typical cherry red spot in the right eye. (B) Increased retinal reflectivity and internal retinal thickness are apparent in spectral domain optical coherence tomography. (C) Transfemoral cerebral angiogram performed 1 day after surgery, showing no definitive occlusion in the ophthalmic artery (arrow) or cerebral arteries.
Cited by 1 articles
-
Central Retinal Artery Occlusion after Trauma: Report of Two Cases
Joong Sik Koh, Se Joon Woo
J Korean Ophthalmol Soc. 2016;57(2):324-329. doi: 10.3341/jkos.2016.57.2.324.
Reference
-
1. Hwang G, Woo SJ, Jung C, et al. Intra-arterial thrombolysis for central retinal artery occlusion: two cases report. J Korean Med Sci. 2010; 25:974–979.2. Park SJ, Choi NK, Seo KH, et al. Nationwide incidence of clinically diagnosed central retinal artery occlusion in Korea, 2008 to 2011. Ophthalmology. 2014; 121:1933–1938.3. Hazin R, Dixon JA, Bhatti MT. Thrombolytic therapy in central retinal artery occlusion: cutting edge therapy, standard of care therapy, or impractical therapy? Curr Opin Ophthalmol. 2009; 20:210–218.4. Ashwin PT, Mirza S, Ajithkumar N, Tsaloumas MD. Iatrogenic central retinal artery occlusion during treatment for epistaxis. Br J Ophthalmol. 2007; 91:122–123.5. Klein ML, Jampol LM, Condon PI, et al. Central retinal artery occlusion without retrobulbar hemorrhage after retrobulbar anesthesia. Am J Ophthalmol. 1982; 93:573–577.6. Li W, Hu Z, Gao R. Iatrogenic central artery embolism. Yan Ke Xue Bao. 1990; 6:102–104.7. Park SW, Woo SJ, Park KH, et al. Iatrogenic retinal artery occlusion caused by cosmetic facial filler injections. Am J Ophthalmol. 2012; 154:653–662.e1.8. Tappeiner C, Garweg JG. Retinal vascular occlusion after vitrectomy with retrobulbar anesthesia-observational case series and survey of literature. Graefes Arch Clin Exp Ophthalmol. 2011; 249:1831–1835.9. Feibel RM. Current concepts in retrobulbar anesthesia. Surv Ophthalmol. 1985; 30:102–110.10. Torres RJ, Luchini A, Weis W, et al. Combined central retinal vein and artery occlusion after retrobulbar anesthesia: report of two cases. Arq Bras Oftalmol. 2005; 68:257–261.11. Giuffre G, Vadala M, Manfre L. Retrobulbar anesthesia complicated by combined central retinal vein and artery occlusion and massive vitreoretinal f ibrosis. Retina. 1995; 15:439–441.12. Sullivan KL, Brown GC, Forman AR, et al. Retrobulbar anesthesia and retinal vascular obstruction. Ophthalmology. 1983; 90:373–377.13. Morgan CM, Schatz H, Vine AK, et al. Ocular complications associated with retrobulbar injections. Ophthalmology. 1988; 95:660–665.14. Mieler WF, Bennett SR, Platt LW, Koenig SB. Localized retinal detachment with combined central retinal artery and vein occlusion after retrobulbar anesthesia. Retina. 1990; 10:278–283.15. Jacobi PC, Dietlein TS, Jacobi FK. A comparative study of topical vs retrobulbar anesthesia in complicated cataract surgery. Arch Ophthalmol. 2000; 118:1037–1043.16. Cowley M, Campochiaro PA, Newman SA, Fogle JA. Retinal vascular occlusion without retrobulbar or optic nerve sheath hemorrhage after retrobulbar injection of lidocaine. Ophthalmic Surg. 1988; 19:859–861.17. Roth SE, Magargal LE, Kimmel AS, et al. Central retinal-artery occlusion in proliferative sickle-cell retinopathy after retrobulbar injection. Ann Ophthalmol. 1988; 20:221–224.18. Mameletzi E, Pournaras JA, Ambresin A, Nguyen C. Retinal embolisation with localised retinal detachment following retrobulbar anaesthesia. Klin Monbl Augenheilkd. 2008; 225:476–478.19. Stewart JM. Mechanism of ophthalmic artery occlusion following pars plana vitrectomy. Br J Ophthalmol. 2003; 87:376.20. Horven I. Ophthalmic artery pressure during retrobulbar anaesthesia. Acta Ophthalmol (Copenh). 1978; 56:574–586.21. Vinerovsky A, Rath EZ, Rehany U, Rumelt S. Central retinal artery occlusion after peribulbar anesthesia. J Cataract Refract Surg. 2004; 30:913–915.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Central Retinal Artery Occlusion Without Retrobular Hemorrhage after Retrobulbar Anesthesia
- Combined Central Retinal Vein and Artery Occlusion After Retrobulbar Anesthesia: A Case Report
- Central Retinal Artery Occlusion after Cervical Spine Surgery in Prone Position: A Case Report
- Central Retinal Artery Occlusion Following General Anesthesia
- Central Retinal Artery Occlusion in Association with Thyroid Ophthalmopathy
