Ann Surg Treat Res.
2016 Dec;91(6):323-326. 10.4174/astr.2016.91.6.323.
Multiple endocrine neoplasia type 1 with anterior mediastinal parathyroid adenoma: successful localization using Tc-99m sestamibi SPECT/CT
- Affiliations
-
- 1Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. iryoo@catholic.ac.kr
- 2Department of Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2360393
- DOI: http://doi.org/10.4174/astr.2016.91.6.323
Abstract
- The most common manifestation of multiple endocrine neoplasia type 1 (MEN1) is hyperparathyroidism. Treatment of hyperparathyroidism in MEN patients is surgical removal of the parathyroid glands, however ectopic parathyroid gland is challenging for treatment. A 51-year-old female, the eldest of 3 MEN1 sisters, had hyperparathyroidism with ectopic parathyroid adenoma in the mediastinal para-aortic region, which was detected by technetium-99m (Tc-99m) sestamibi scintigraphy and single-photon emission computed tomography/computed tomography (SPECT/CT). She underwent total parathyroidectomy with video-assisted thoracoscopic surgery on an anterior mediastinal mass. Anterior mediastinal parathyroid adenoma in MEN1 patients is rare. Precise localization of an ectopic parathyroid gland with Tc-99m sestamibi SPECT/CT can lead to successful treatment of hyperparathyroidism. This is the first reported case in the literature of mediastinal parathyroid adenoma in MEN1 patient visualized by Tc-99m sestamibi SPECT/CT.
Keyword
MeSH Terms
Figure
-
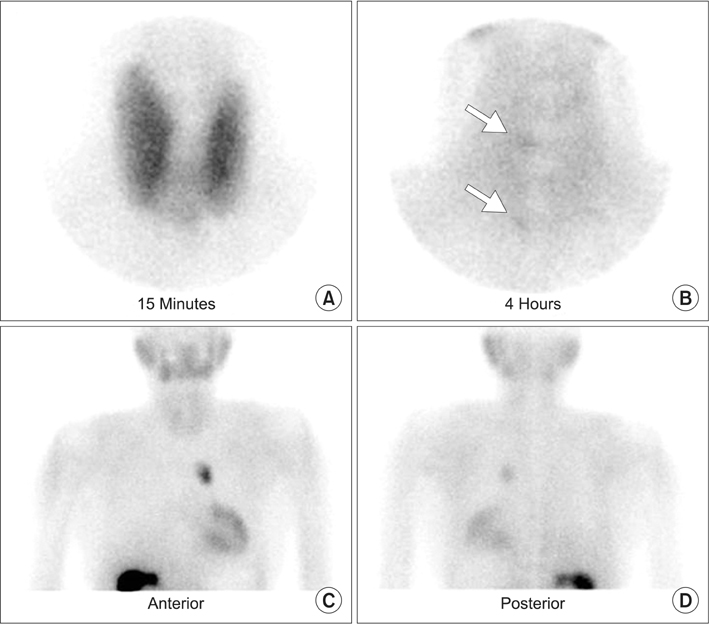
Fig. 1 Technetium-99m sestamibi scan. (A) On early 15-minute image of anterior neck, diffuse thyroid activity is seen. (B) On late 4-hour image, thyroidal activity is washed out and small focal uptake areas are noted in upper and lower portion of right thyroid bed (arrows). (C, D) On the chest planar image for excluding ectopic parathyroid gland, focal hot uptake is noted in mid chest region.

Fig. 2 Technetium-99m sestamibi single-photon emission computed tomography/computed tomography (SPECT/CT). (A) Focal hot uptake is noted in anterior mediastinum on SPECT image. (B, C) A lobulated nodular lesion with increased sestamibi uptake is seen in left paraaortic region on CT and SPECT/CT images.
Reference
-
1. Kivlen MH, Bartlett DL, Libutti SK, Skarulis MC, Marx SJ, Simonds WF, et al. Reoperation for hyperparathyroidism in multiple endocrine neoplasia type 1. Surgery. 2001; 130:991–998.2. Lavely WC, Goetze S, Friedman KP, Leal JP, Zhang Z, Garret-Mayer E, et al. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. J Nucl Med. 2007; 48:1084–1089.3. Thakker RV. Multiple endocrine neoplasia type 1 (MEN1). Best Pract Res Clin Endocrinol Metab. 2010; 24:355–370.4. Thakker RV. Multiple endocrine neoplasia: syndromes of the twentieth century. J Clin Endocrinol Metab. 1998; 83:2617–2620.5. Benson L, Ljunghall S, Akerstrom G, Oberg K. Hyperparathyroidism presenting as the first lesion in multiple endocrine neoplasia type 1. Am J Med. 1987; 82:731–737.6. Burgess JR, David R, Greenaway TM, Parameswaran V, Shepherd JJ. Osteoporosis in multiple endocrine neoplasia type 1: severity, clinical significance, relationship to primary hyperparathyroidism, and response to parathyroidectomy. Arch Surg. 1999; 134:1119–1123.7. Tonelli F, Marcucci T, Fratini G, Tommasi MS, Falchetti A, Brandi ML. Is total parathyroidectomy the treatment of choice for hyperparathyroidism in multiple endocrine neoplasia type 1? Ann Surg. 2007; 246:1075–1082.8. Eslamy HK, Ziessman HA. Parathyroid scintigraphy in patients with primary hyperparathyroidism: 99mTc sestamibi SPECT and SPECT/CT. Radiographics. 2008; 28:1461–1476.9. Flint PW, Haughey BH, Lund VJ, Niparko JK, Robbins KT, Thomas JR, et al. Cummings otolaryngology: head and neck surgery. 6th ed.Philadelphia (PA): Elsevier/Saunders;2015.10. Arnalsteen LC, Alesina PF, Quiereux JL, Farrel SG, Patton FN, Carnaille BM, et al. Long-term results of less than total parathyroidectomy for hyperparathyroidism in multiple endocrine neoplasia type 1. Surgery. 2002; 132:1119–1124.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mediastinal parathyroid adenoma localized by technetium-99m sestamibi scanning
- Ectopic Mediastinal Parathyroid Adenoma in a Patient with Chronic Kidney Disease: A Case Report
- Primary Hyperparathyroidism with Ectopic Parathyroid Adenoma Detected by Both 99mTc-MIBI SPECT and Contrast-Enhanced Neck CT
- False-Positive Parathyroid Sestamibi in Minimally Invasive Radioguided Parathyroidectomy
- A case of mediastinal parathyroid adenoma presenting as fracture of brown tumor
