Anesth Pain Med.
2016 Apr;11(2):182-185. 10.17085/apm.2016.11.2.182.
Increased amount of pleural effusion during head-down tilt position in ovarian cancer patient with ascites: A case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Daegu Fatima Hospital, Daegu, Korea. sym0712@nate.com
- KMID: 2358482
- DOI: http://doi.org/10.17085/apm.2016.11.2.182
Abstract
- Pseudo-Meigs syndrome is accompanied with pleural effusion, ascites and a benign or malignant tumor of ovary, tubes, uterus, round ligament or colon. We reported a case of hypoxia in an ovarian cancer patient with moderate ascites after head-down tilt position for central venous catheterization under general anesthesia. Massive pleural effusion was detected on portable chest X-ray, which was not observed in a preoperative radiologic test. The patient had no respiratory symptoms and breath sound was normal in both lungs prior to surgery. The pleural effusion was resolved by a chest tube insertion.
Keyword
MeSH Terms
Figure
-

Fig. 1 Pelvic computed tomography shows huge pelvic mass, suggestive ovarian mass and moderate ascites.
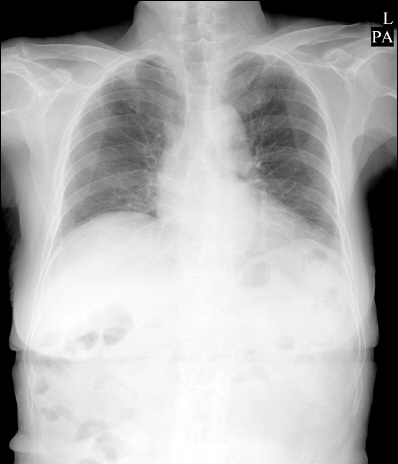
Fig. 2 Chest radiograph 12 days before surgery shows no evidence of the active pulmonary lesion.

Fig. 3 Abdomen CT 12 days before surgery shows extremely small amount of pleural effusion on right lower lung field.

Fig. 4 Portable chest radiograph after head-down tilt position shows massive pleural effusion in right lung field.

Fig. 5 Chest radiograph 1 day after chest tube insertion shows normal finding.
Reference
-
1. Meigs JV. Pelvic tumors other than fibromas of the ovary with ascites and hydrothorax. Obstet Gynecol. 1954; 3:471–86.
Article2. Meigs JV. Fibroma of the ovary with ascites and hydrothorax: a further report. Ann Surg. 1939; 110:731–54. DOI: 10.1097/00000658-193910000-00019. PMID: 17857484. PMCID: PMC1391413.3. Iavazzo C, Vorgias G, Sampanis D, Mavromatis I, Manikis P, Katsoulis M. Meig’s or Pseudomeig’s syndrome? Bratisl Lek Listy. 2007; 108:158–60.4. Samanth KK, Black WC 3rd. Benign ovarian stromal tumors associated with free peritoneal fluid. Am J Obstet Gynecol. 1970; 107:538–45.
Article5. Kirschner PA. Porous diaphragm syndromes. Chest Surg Clin N Am. 1998; 8:449–72.6. Okuyama T, Kimura M, Uchida J, Nishino K, Kumagai T, Fujiwara A, et al. Porous diaphragm syndrome with repeated rapid accumulation of pleural effusion. Intern Med. 2014; 53:1075–7. DOI: 10.2169/internalmedicine.53.1444. PMID: 24827488.
Article7. Lew SQ. Hydrothorax: pleural effusion associated with peritoneal dialysis. Perit Dial Int. 2010; 30:13–8. DOI: 10.3747/pdi.2008.00168. PMID: 20056973.
Article8. Papanikolaou C, Fortounis K, Ainalis S, Biba K, Papanikolaou A, Hatzitheoxaris G. Pseudo-Meigs syndrome: a case report. Internet J Pathol. 2004. 4:Available from http://ispub.com/IJPA/4/2/13378.
Article9. Ravindran J. Massive ovarian cysts--successful management of two cases. Med J Malaysia. 1994; 49:303–5. PMID: 7845287.10. Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology. 2004; 100:9–15. DOI: 10.1097/00000542-200401000-00006. PMID: 14695718.
Article11. Kanno T, Yoshikawa D, Tomioka A, Kamijyo T, Yamada K, Goto F. Hydrothorax: an unexpected complication after laparoscopic myomectomy. Br J Anaesth. 2001; 87:507–9. DOI: 10.1093/bja/87.3.507. PMID: 11517142.
Article
