Endoscopic Management of Gastroesophageal Reflux Disease: Revisited
- Affiliations
-
- 1Asian Institute of Gastroenterology, Hyderabad, India. aigindia@yahoo.co.in
- KMID: 2356044
- DOI: http://doi.org/10.5946/ce.2016.133
Abstract
- Gastroesophageal reflux disease (GERD) is defined by the presence of troublesome symptoms resulting from the reflux of gastric contents. The prevalence of GERD is increasing globally. An incompetent lower esophageal sphincter underlies the pathogenesis of GERD. Proton pump inhibitors (PPIs) form the core of GERD management. However, a substantial number of patients do not respond well to PPIs. The next option is anti-reflux surgery, which is efficacious, but it has its own limitations, such as gas bloating, inability to belch or vomit, and dysphagia. Laparoscopic placement of magnetic augmentation device is emerging as a useful alternative to conventional anti-reflux surgery. However, invasiveness of a surgical procedure remains a concern for the patients. The proportion of PPI non-responders or partial responders who do not wish for anti-reflux surgery defines the "˜treatment gap' and needs to be addressed. The last decade has witnessed the fall and rise of many endoscopic devices for GERD. Major endoscopic strategies include radiofrequency ablation and endoscopic fundoplication devices. Current endoscopic devices score high on subjective improvement, but have been unimpressive in objective improvement like esophageal acid exposure. In this review, we discuss the current endoscopic anti-reflux therapies and available evidence for their role in the management of GERD.
MeSH Terms
Figure
-

Fig. 1. Currently available endoscopic anti-reflux modalities. Stretta (Mederi Therapeutics), EsophyX (EndoGastric Solutions), MUSE (Medigus), GERDx (G-SURG GmbH).
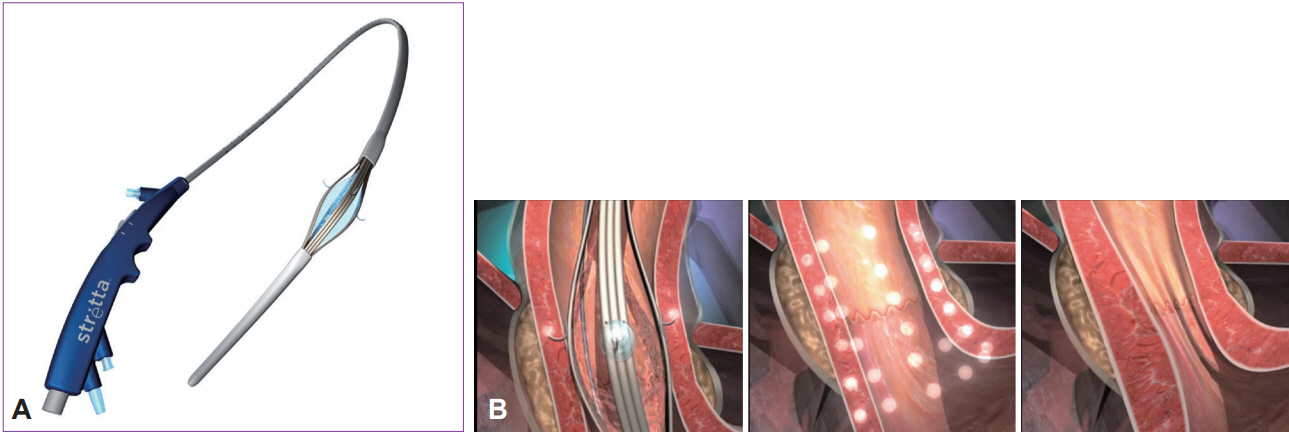
Fig. 2. (A) Radiofrequency device (Stretta; Mederi Therapeutics) with a four-needle balloon catheter system. (B) Depiction of Stretta procedure-radiofrequency energy delivered to gastroesophageal junction muscle at multiple sites.
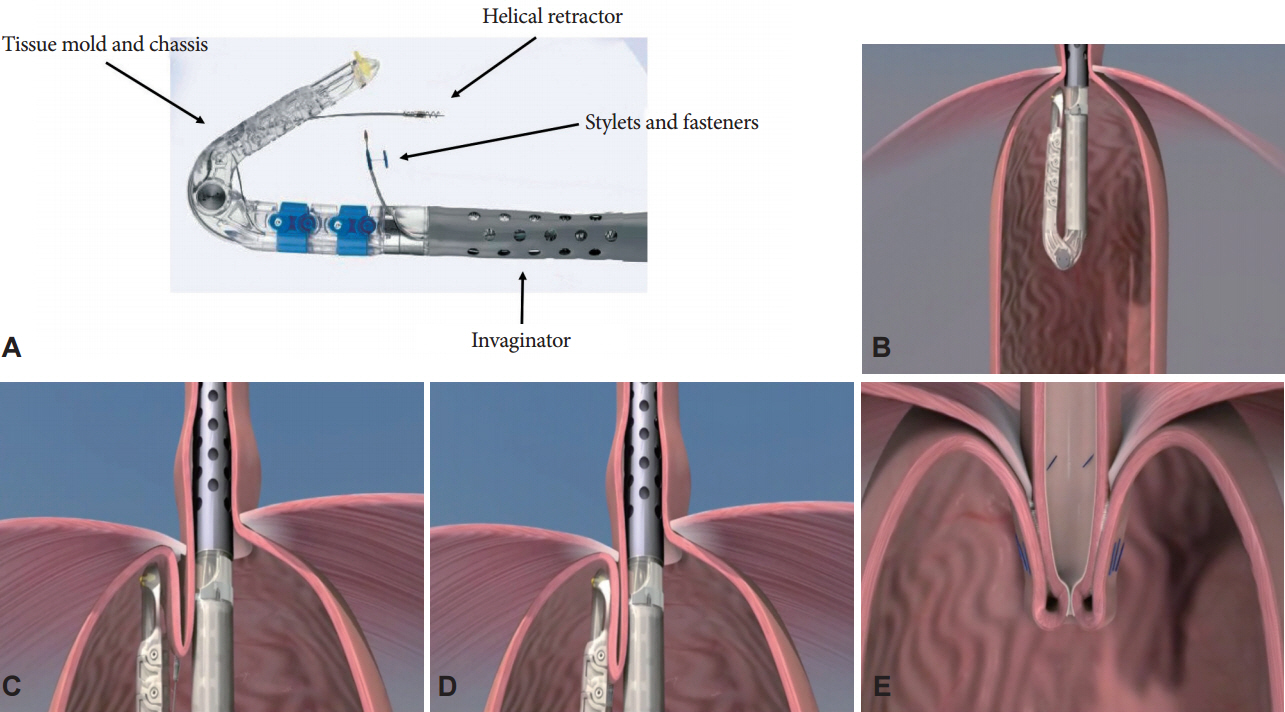
Fig. 3. (A) Transoral fundoplication device (EsophyX; EndoGastric Solutions) and its components. (B) Retroflexed device in the stomach. (C) Engaging the helical retractor into the tissue. (D) Application of H-shaped polypropylene fasteners (about 20). (E) Creation of full-thickness partial circumference fundoplication.
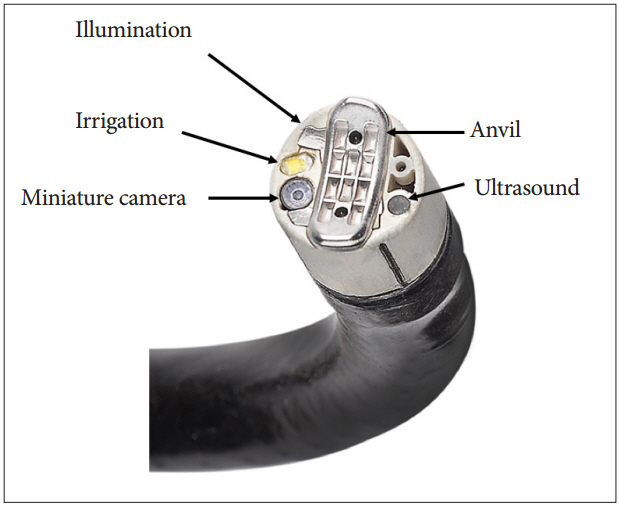
Fig. 4. MUSE (Medigus) endoscopic stapling device and its components.

Fig. 5. (A, B) Full thickness endoscopic plication device (GERDx; G-SURG GmbH). (C) GERDx inside the stomach in retroflexed view. (D) Advancement of ‘Drill helix’ into gastric cardia. (E) Closure of the device arms after gathering tissue and deployment of suture. (F) Reopening of the device arms after plication implant.
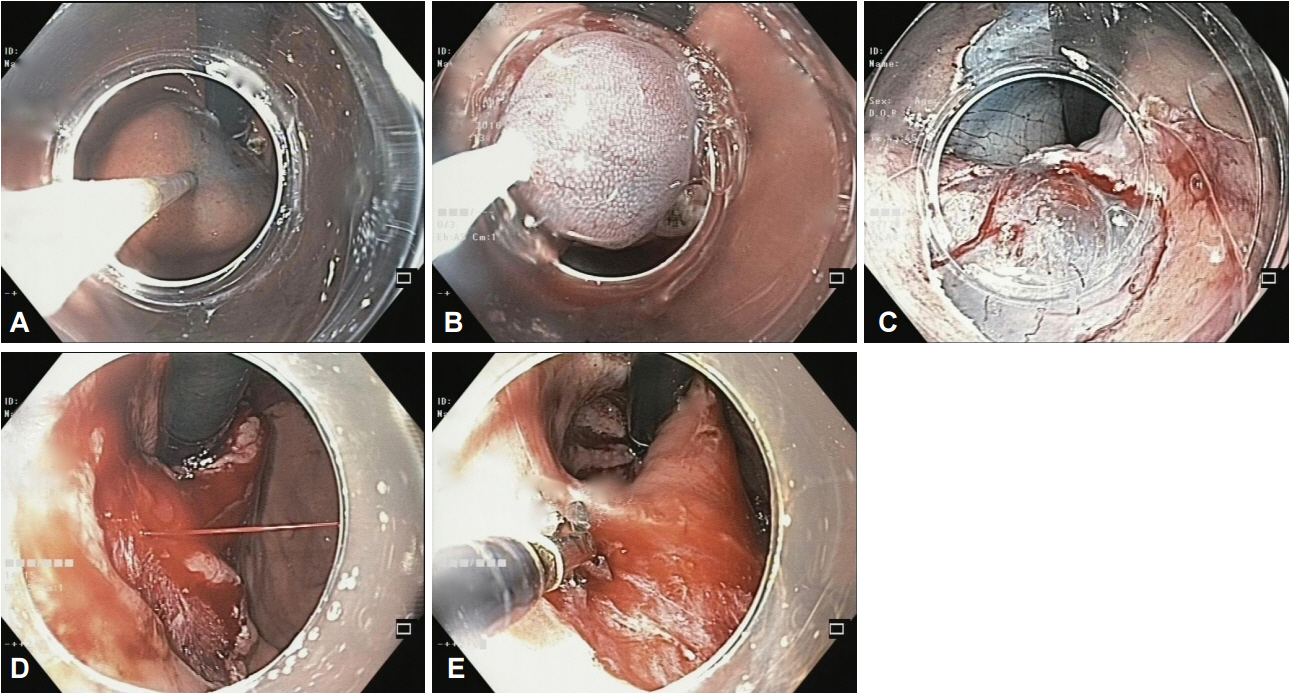
Fig. 6. (A) Submucosal injection of saline with indigo-carmine at gastric cardia. (B) Application of snare over the mucosa with cap-endoscopic mucosal resection technique. (C) Completion of near circumferential (2/3) resection of gastric mucosa. (D) Actively bleeding spurter during mucosectomy procedure. (E) Effective control of bleeding vessel with coagrasper.
Reference
-
1. El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014; 63:871–880.
Article2. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2013; 108:308–328.
Article3. Lazarus B, Chen Y, Wilson FP, et al. Proton pump inhibitor use and the risk of chronic kidney disease. JAMA Intern Med. 2016; 176:238–246.
Article4. Abraham NS. Proton pump inhibitors: potential adverse effects. Curr Opin Gastroenterol. 2012; 28:615–620.5. Schoenfeld AJ, Grady D. Adverse effects associated with proton pump inhibitors. JAMA Intern Med. 2016; 176:172–174.
Article6. Broeders JA, Rijnhart-de Jong HG, Draaisma WA, Bredenoord AJ, Smout AJ, Gooszen HG. Ten-year outcome of laparoscopic and conventional nissen fundoplication: randomized clinical trial. Ann Surg. 2009; 250:698–706.7. Du X, Hu Z, Yan C, Zhang C, Wang Z, Wu J. A meta-analysis of long follow-up outcomes of laparoscopic Nissen (total) versus Toupet (270 degrees) fundoplication for gastro-esophageal reflux disease based on randomized controlled trials in adults. BMC Gastroenterol. 2016; 16:88.
Article8. Galmiche JP, Hatlebakk J, Attwood S, et al. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial. JAMA. 2011; 305:1969–1977.
Article9. Ganz RA, Peters JH, Horgan S, et al. Esophageal sphincter device for gastroesophageal reflux disease. N Engl J Med. 2013; 368:719–727.
Article10. Zhang H, Dong D, Liu Z, He S, Hu L, Lv Y. Revaluation of the efficacy of magnetic sphincter augmentation for treating gastroesophageal reflux disease. Surg Endosc. 2016; 30:3684–3690.
Article11. Bauer M, Meining A, Kranzfelder M, et al. Endoluminal perforation of a magnetic antireflux device. Surg Endosc. 2015; 29:3806–3810.
Article12. Kim MS, Holloway RH, Dent J, Utley DS. Radiofrequency energy delivery to the gastric cardia inhibits triggering of transient lower esophageal sphincter relaxation and gastroesophageal reflux in dogs. Gastrointest Endosc. 2003; 57:17–22.
Article13. Tam WC, Schoeman MN, Zhang Q, et al. Delivery of radiofrequency energy to the lower oesophageal sphincter and gastric cardia inhibits transient lower oesophageal sphincter relaxations and gastro-oesophageal reflux in patients with reflux disease. Gut. 2003; 52:479–485.
Article14. Arts J, Bisschops R, Blondeau K, et al. A double-blind sham-controlled study of the effect of radiofrequency energy on symptoms and distensibility of the gastro-esophageal junction in GERD. Am J Gastroenterol. 2012; 107:222–230.
Article15. Aziz AM, El-Khayat HR, Sadek A, et al. A prospective randomized trial of sham, single-dose Stretta, and double-dose Stretta for the treatment of gastroesophageal reflux disease. Surg Endosc. 2010; 24:818–825.
Article16. Dughera L, Rotondano G, De Cento M, Cassolino P, Cisarò F. Durability of Stretta radiofrequency treatment for GERD: results of an 8-year follow-up. Gastroenterol Res Pract. 2014; 2014:531907.
Article17. Corley DA, Katz P, Wo JM, et al. Improvement of gastroesophageal reflux symptoms after radiofrequency energy: a randomized, sham-controlled trial. Gastroenterology. 2003; 125:668–676.
Article18. Coron E, Sebille V, Cadiot G, et al. Clinical trial: radiofrequency energy delivery in proton pump inhibitor-dependent gastro-oesophageal reflux disease patients. Aliment Pharmacol Ther. 2008; 28:1147–1158.
Article19. Noar M, Squires P, Noar E, Lee M. Long-term maintenance effect of radiofrequency energy delivery for refractory GERD: a decade later. Surg Endosc. 2014; 28:2323–2333.
Article20. Perry KA, Banerjee A, Melvin WS. Radiofrequency energy delivery to the lower esophageal sphincter reduces esophageal acid exposure and improves GERD symptoms: a systematic review and meta-analysis. Surg Laparosc Endosc Percutan Tech. 2012; 22:283–288.21. Auyang ED, Carter P, Rauth T, Fanelli RD; SAGES Guidelines Committee. SAGES clinical spotlight review: endoluminal treatments for gastroesophageal reflux disease (GERD). Surg Endosc. 2013; 27:2658–2672.
Article22. Lipka S, Kumar A, Richter JE. No evidence for efficacy of radiofrequency ablation for treatment of gastroesophageal reflux disease: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2015; 13:1058–1067. e1.
Article23. Richardson WS, Stefanidis D, Fanelli RD. Society of American Gastrointestinal and Endoscopic Surgeons response to “no evidence for efficacy of radiofrequency ablation for treatment of gastroesophageal reflux disease: a systematic review and meta-analysis”. Clin Gastroenterol Hepatol. 2015; 13:1700–1701.
Article24. Liang WT, Yan C, Wang ZG, et al. Early and midterm outcome after laparoscopic fundoplication and a minimally invasive endoscopic procedure in patients with gastroesophageal reflux disease: a prospective observational study. J Laparoendosc Adv Surg Tech A. 2015; 25:657–661.
Article25. Yan C, Liang WT, Wang ZG, et al. Comparison of Stretta procedure and toupet fundoplication for gastroesophageal reflux disease-related extra-esophageal symptoms. World J Gastroenterol. 2015; 21:12882–12887.
Article26. Liang WT, Wu JM, Wang F, Hu ZW, Wang ZG. Stretta radiofrequency for gastroesophageal reflux disease-related respiratory symptoms: a prospective 5-year study. Minerva Chir. 2014; 69:293–299.27. Zhang C, Wu J, Hu Z, et al. Diagnosis and anti-reflux therapy for GERD with respiratory symptoms: a study using multichannel intraluminal impedance-pH monitoring. PLoS One. 2016; 11:e0160139.
Article28. Pandolfino JE, Krishnan K. Do endoscopic antireflux procedures fit in the current treatment paradigm of gastroesophageal reflux disease? Clin Gastroenterol Hepatol. 2014; 12:544–554.
Article29. Hunter JG, Kahrilas PJ, Bell RC, et al. Efficacy of transoral fundoplication vs omeprazole for treatment of regurgitation in a randomized controlled trial. Gastroenterology. 2015; 148:324–333. e5.
Article30. Trad KS, Barnes WE, Simoni G, et al. Transoral incisionless fundoplication effective in eliminating GERD symptoms in partial responders to proton pump inhibitor therapy at 6 months: the TEMPO Randomized Clinical Trial. Surg Innov. 2015; 22:26–40.31. Trad KS, Simoni G, Barnes WE, et al. Efficacy of transoral fundoplication for treatment of chronic gastroesophageal reflux disease incompletely controlled with high-dose proton-pump inhibitors therapy: a randomized, multicenter, open label, crossover study. BMC Gastroenterol. 2014; 14:174.
Article32. Håkansson B, Montgomery M, Cadiere GB, et al. Randomised clinical trial: transoral incisionless fundoplication vs. sham intervention to control chronic GERD. Aliment Pharmacol Ther. 2015; 42:1261–1270.
Article33. Testoni PA, Mazzoleni G, Testoni SG. Transoral incisionless fundoplication for gastro-esophageal reflux disease: techniques and outcomes. World J Gastrointest Pharmacol Ther. 2016; 7:179–189.
Article34. Huang X, Chen S, Zhao H, et al. Efficacy of transoral incisionless fundoplication (TIF) for the treatment of GERD: a systematic review with meta-analysis. Surg Endosc. 2016; Aug. 5. [Epub]. http://dx.doi.org/10.1007/s00464-016-5111-7.
Article35. Testoni PA, Testoni S, Mazzoleni G, Vailati C, Passaretti S. Long-term efficacy of transoral incisionless fundoplication with Esophyx (Tif 2.0) and factors affecting outcomes in GERD patients followed for up to 6 years: a prospective single-center study. Surg Endosc. 2015; 29:2770–2780.36. Toomey P, Teta A, Patel K, Ross S, Sukharamwala P, Rosemurgy AS. Transoral incisionless fundoplication: is it as safe and efficacious as a Nissen or Toupet fundoplication? Am Surg. 2014; 80:860–867.
Article37. Bell RC, Fox MA, Barnes WE, et al. Univariate and multivariate analyses of preoperative factors influencing symptomatic outcomes of transoral fundoplication. Surg Endosc. 2014; 28:2949–2958.
Article38. Witteman BP, Kessing BF, Snijders G, Koek GH, Conchillo JM, Bouvy ND. Revisional laparoscopic antireflux surgery after unsuccessful endoscopic fundoplication. Surg Endosc. 2013; 27:2231–2236.
Article39. Jain D, Singhal S. Transoral incisionless fundoplication for refractory gastroesophageal reflux disease: where do we stand? Clin Endosc. 2016; 49:147–156.
Article40. Zacherl J, Roy-Shapira A, Bonavina L, et al. Endoscopic anterior fundoplication with the Medigus Ultrasonic Surgical Endostapler (MUSE) for gastroesophageal reflux disease: 6-month results from a multi-center prospective trial. Surg Endosc. 2015; 29:220–229.
Article41. Kim HJ, Kwon CI, Kessler WR, et al. Long-term follow-up results of endoscopic treatment of gastroesophageal reflux disease with the MUSE endoscopic stapling device. Surg Endosc. 2016; 30:3402–3408.
Article42. Gweon TG, Matthes K. Prospective, randomized ex vivo trial to assess the ideal stapling site for endoscopic fundoplication with medigus ultrasonic surgical endostapler. Gastroenterol Res Pract. 2016; 2016:3161738.
Article43. Pace F, Costamagna G, Penagini R, Repici A, Annese V. Review article: endoscopic antireflux procedures: an unfulfilled promise? Aliment Pharmacol Ther. 2008; 27:375–384.44. Koch OO, Kaindlstorfer A, Antoniou SA, Spaun G, Pointner R, Swanstrom LL. Subjective and objective data on esophageal manometry and impedance pH monitoring 1 year after endoscopic full-thickness plication for the treatment of GERD by using multiple plication implants. Gastrointest Endosc. 2013; 77:7–14.
Article45. von Renteln D, Schiefke I, Fuchs KH, et al. Endoscopic full-thickness plication for the treatment of gastroesophageal reflux disease using multiple Plicator implants: 12-month multicenter study results. Surg Endosc. 2009; 23:1866–1875.
Article46. von Renteln D, Schiefke I, Fuchs KH, et al. Endoscopic full-thickness plication for the treatment of GERD by application of multiple Plicator implants: a multicenter study (with video). Gastrointest Endosc. 2008; 68:833–844.
Article47. Satodate H, Inoue H, Fukami N, Shiokawa A, Kudo SE. Squamous reepithelialization after circumferential endoscopic mucosal resection of superficial carcinoma arising in Barrett’s esophagus. Endoscopy. 2004; 36:909–912.
Article48. Inoue H, Ito H, Ikeda H, et al. Anti-reflux mucosectomy for gastroesophageal reflux disease in the absence of hiatus hernia: a pilot study. Ann Gastroenterol. 2014; 27:346–351.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Bariatric Surgery and Endoscopic Procedures on Gastroesophageal Reflux Disease
- Upper Gastrointestinal Cancer and Reflux Disease
- Radiologic studies on gastroesophageal reflux
- How Is the Autonomic Nerve Function Different Between Gastroesophageal Reflux Disease Alone and Gastroesophageal Reflux Disease With Diabetes Mellitus Neuropathy?
- Endoscopic Accessories Used for More Advanced Endoluminal Therapeutic Procedures
