Treatment of a Giant Serpentine Aneurysm in the Anterior Cerebral Artery
- Affiliations
-
- 1Department of Neurosurgery, Busan Paik Hospital, Inje University, School of Medicine, Busan, Korea.
- 2Department of Diagnostic Radiology, Busan Paik Hospital, Inje University, School of Medicine, Busan, Korea. hwjeong2000@lycos.co.kr
- KMID: 2354891
- DOI: http://doi.org/10.7461/jcen.2016.18.2.141
Abstract
- A giant serpentine aneurysm (GSA) in the anterior cerebral artery (ACA) poses a technical challenge in treatment given its large size, unique neck, and dependent distal vessels. Here we report the case of a GSA in the ACA successfully treated with a combined surgical and endovascular approach. A 54-year-old woman presented with dull headache. On brain computed tomography (CT), a large mass (7 cm × 5 cm × 5 cm) was identified in the left frontal lobe. Cerebral angiography revealed a GSA in the left ACA. Bypass surgery of the distal ACA was performed, followed byocclusion of the entry channel via an endovascular approach. Follow-up CT performed 5 days after treatment revealed disappearance of the vascular channel and peripheral rim enhancement. Follow-up imaging studies performed 7 months after treatment revealed gradual reduction of the mass effect and patency of bypass flow. No complications were noted over a period of 1 year after surgery.
MeSH Terms
Figure
-
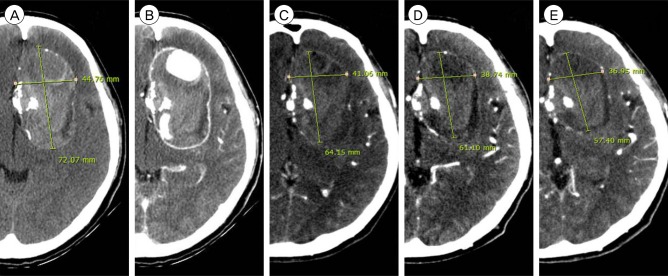
Fig. 1 (A, B) Initial brain computed tomography images showing a heterogeneous large mass (7 cm × 5 cm × 5 cm) with central and rim enhancements (A: non-enhanced axial image; B: enhanced axial image). (C) Five days after treatment. Follow-up brain computed tomography axial view showing disappearance of the vascular channel and peripheral rim enhancement. (D) Four months after treatment.Axial view showing reduction of the mass effect. (E) Seven months after treatment. Axial view showing further reduction of the mass effect.
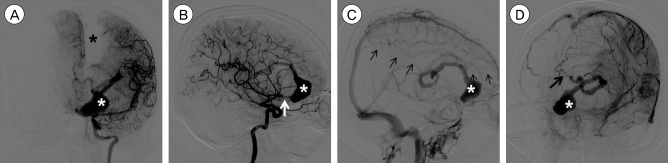
Fig. 2 Internal carotid artery angiography images. (A) Anteroposterior view in the arterial phase showing a giant serpentine aneurysm (GSA) and filling defect of the left distal anterior cerebral artery (ACA) territory (black asterisk: left distal ACA filling defect; white asterisk: GSA lumen with contrast filling). (B) Lateral view in the arterial phase showing a GSA and entry channel (white arrow: entry point of the GSA). (C) Lateral view in the late venous phase showing delayed filling of the left distal ACA territory (small black arrows: territory of the left distal ACA). (D) Oblique view in the late venous phase showing the exit channel of the GSA (black arrow: exit channel of the GSA).
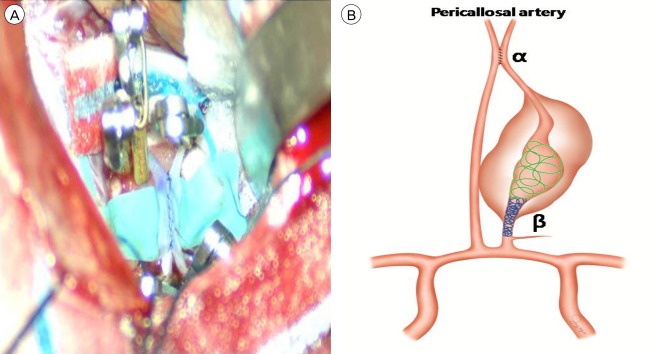
Fig. 3 (A) The condition after bypass and before temporary clip removal. (B) Schematic drawing of the treatment plan for the giant serpentine aneurysm (GSA) in the distal anterior cerebral artery (ACA). α: In situ "side-to-side" bypass of both distal ACAs, β: Occlusion of the entry channel via an endovascular approach using detachable coils. Occlusion is performed in 2 steps. First, the distal widest part of the GSA is loosely packed using large coils (green helix). Second, the proximal narrow part between the distal perforator of the feeding artery and the beginning of the aneurysm is densely packed using coils (blue helix).
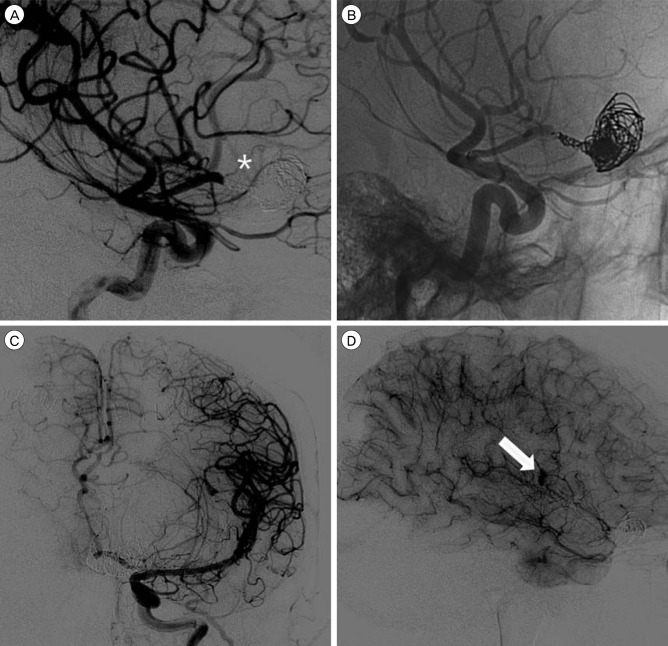
Fig. 4 (A) Lateral view of the working angle after endovascular occlusion showing that the perforating artery is not sacrificed (asterisk indicates the perforating artery). (B) Native view of the working angle showing a loosely packed distal part and densely packed proximal part of thegiant serpentine aneurysm (GSA). (C) Left internal carotid artery angiography in the late arterial phase (anteroposterior view) after entry channel occlusion showing a GSA and patient collateral flow via bypass. (D) Left internal carotid artery angiographyin the capillary phase (lateral view) after entry channel occlusion showing retrograde contrast filling of the GSA (the white arrow indicates retrograde contrast filling).
Reference
-
1. Abla AA, Lawton MT. Anterior cerebral artery bypass for complex aneurysms: An experience with intracranial-intracranial reconstruction and review of bypass options. J Neurosurg. 2014; 6. 120(6):1364–1377. PMID: 24745711.
Article2. Aletich VA, Debrun GM, Monsein LH, Nauta HJ, Spetzler RF. Giant serpentine aneurysms: A review and presentation of five cases. AJNR Am J Neuroradiol. 1995; 5. 16(5):1061–1072. PMID: 7639128.3. Amin-Hanjani S, Chen PR, Chang SW, Spetzler RF. Long-term follow-up of giant serpentine MCA aneurysm treated with EC-IC bypass and proximal occlusion. Acta Neurochir (Wien). 2006; 2. 148(2):227–228. PMID: 16322902.
Article4. Carlson AP. Tailored PICA revascularization for unusual ruptured fusiform vertebro-PICA origin aneurysms: Rationale and case illustrations. J Neurol Surg Rep. 2015; 11. 76(2):e275–e278. PMID: 26623241.
Article5. Christiano LD, Gupta G, Prestigiacomo CJ, Gandhi CD. Giant serpentine aneurysms. Neurosurg Focus. 2009; 5. 26(5):E5.
Article6. Dunn GP, Gerrard JL, Jho DH, Ogilvy CS. Surgical treatment of a large fusiform distal anterior cerebral artery aneurysm with in situ end-to-side A3-A3 bypass graft and aneurysm trapping: Case report and review of the literature. Neurosurgery. 2011; 2. 68(2):E587–E591. discussion E591. PMID: 21135720.7. Fanning NF, Kelleher MO, Ryder DQ. The pretzel sign: Angiographic pattern of tortuous intra-aneurysmal blood flow in a giant serpentine aneurysm. Br J Neurosurg. 2003; 2. 17(1):67–71. PMID: 12779205.
Article8. Ferroli P, Ciceri E, Addis A, Broggi G. Self-closing surgical clips for use in pericallosal artery-pericallosal artery side-to-side bypass. J Neurosurg. 2008; 8. 109(2):330–334. PMID: 18671649.
Article9. Horowitz MB, Yonas H, Jungreis C, Hung TK. Management of a giant middle cerebral artery fusiform serpentine aneurysm with distal clip application and retrograde thrombosis: Case report and review of the literature. Surg Neurol. 1994; 3. 41(3):221–225. PMID: 8146737.
Article10. Ikeda A, Shibuya M, Okada T, Kageyama N. Microvascular side-to-side anastomosis. basic problems and clinical applications. Neurol Med Chir (Tokyo). 1986; 5. 26(5):379–384. PMID: 2429217.11. Lawton MT, Hamilton MG, Morcos JJ, Spetzler RF. Revascularization and aneurysm surgery: Current techniques, indications, and outcome. Neurosurgery. 1996; 1. 38(1):83–92. discussion 92-4. PMID: 8747955.
Article12. Lehecka M, Dashti R, Hernesniemi J, Niemela M, Koivisto T, Ronkainen A, et al. Microneurosurgical management of aneurysms at A3 segment of anterior cerebral artery. Surg Neurol. 2008; 8. 70(2):135–151. discussion 152. PMID: 18482754.
Article13. Otsuka G, Miyachi S, Handa T, Negoro M, Okamoto T, Suzuki O. Endovascular trapping of giant serpentine aneurysms by using guglielmi detachable coils: Successful reduction of mass effect. report of two cases. J Neurosurg. 2001; 5. 94(5):836–840. PMID: 11354420.14. Park ES, Ahn JS, Park JC, Kwon DH, Kwun BD, Kim CJ. STA-ACA bypass using the contralateral STA as an interposition graft for the treatment of complex ACA aneurysms: Report of two cases and a review of the literature. Acta Neurochir (Wien). 012; 8. 154(8):1447–1453. PMID: 22692589.
Article15. Segal HD, McLaurin RL. Giant serpentine aneurysm. report of two cases. J Neurosurg. 1977; 1. 46(1):115–120. PMID: 830809.16. Suzuki S, Takahashi T, Ohkuma H, Shimizu T, Fujita S. Management of giant serpentine aneurysms of the middle cerebral artery--review of literature and report of a case successfully treated by STA-MCA anastomosis only. Acta Neurochir (Wien). 1992; 117(1-2):23–29. PMID: 1514425.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Serpentine Aneurysm of the Middle Cerebral Artery
- Giant Serpentine Intracranial Aneurysm Treated with Wrapping under the Extracorporeal Circulation and Hypothermia
- Giant Serpentine Aneurysm of the Anterior Communicating Artery: Case Report
- Surgical Treatment of Giant Serpentine Aneurysm of A2-A3 Segment Distal Anterior Cerebral Artery : Technical Case Report
- Giant Serpentine Aneurysm of the Posterior Cerebral Artery: Case Report
