Polyostotic Fibrous Dysplasia Mimicking Multiple Bone Metastases in a Patient with Ductal Carcinoma In Situ
- Affiliations
-
- 1Division of Breast and Endocrine Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jeongeon.lee@samsung.com
- 2Department of Surgery, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Department of Nuclear Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Abstract
- Whole-body bone scans and whole body 18F-fluorodeoxyglucose positron emission tomographic/computed tomographic scans are sensitive for detecting bone metastasis in patients with breast cancer. However, it is often difficult to discriminate between bone metastasis and other nonmalignant bone lesions. Polyostotic fibrous dysplasia is a rare disorder characterized by the osteoid medullary cavity filling with fibrous tissue causing bony expansion. We report the case of a 42-year-old female patient with ductal carcinoma in situ, which appeared to have multiple bone metastases on initial work-up images. Subsequently, the bone metastases were identified as polyostotic fibrous dysplasia. The patient underwent modified radical mastectomy and subsequently visited for a second opinion regarding the bony metastases. She underwent right ilium computed tomography-guided biopsy. Pathology was consistent with fibrous dysplasia. This patient received only adjuvant tamoxifen, and 1.5 years later, there was no evidence of recurrence.
Keyword
MeSH Terms
-
Adult
Biopsy
Breast Neoplasms
Carcinoma, Ductal*
Carcinoma, Intraductal, Noninfiltrating*
Electrons
Female
Fibrous Dysplasia of Bone
Fibrous Dysplasia, Polyostotic*
Humans
Ilium
Mastectomy, Modified Radical
Neoplasm Metastasis*
Pathology
Positron-Emission Tomography
Recurrence
Referral and Consultation
Tamoxifen
Whole Body Imaging
Tamoxifen
Figure
-

Figure 1 The chest X-ray as a baseline study for general anesthesia. Osteolytic lesions of the right second, third, eighth, and left fourth ribs, which is suggestive of multiple bone metastases.

Figure 2 The baseline whole body bone scan. Abnormal increased uptake was demonstrated in the right parietal, occipital, cervical, thoracic, lumbar, sacral spine, bilateral scapulae, multiple ribs, bilateral pelvic bones, right femur, tibia, fibula, right tarsal bone, sternum, and right humerus.

Figure 3 Microscopic examination of breast tumor. Cribriform-tumor clusters, with architectural and nuclear atypia, consistent with ductal carcinoma in situ (A, H&E stain, ×40; B, H&E stain, ×200).

Figure 4 Microscopic examination of biopsied specimen of the right ilium. Photomicrograph was demonstrated irregularly shaped islands of woven bone with a bland spindle cell background stroma (H&E stain, ×200).

Figure 5 Follow-up bone scan after 1 year. Increased radio-uptake in the skull, right second, third, fourth, sixth, eighth, and left fourth ribs, right ilium, right ischium, right acetabulum, right femur, right tibia, right fibula, and second phalanx of right foot, which is suggestive of polyostotic fibrous dysplasia, but which cannot exclude combined metastasis.
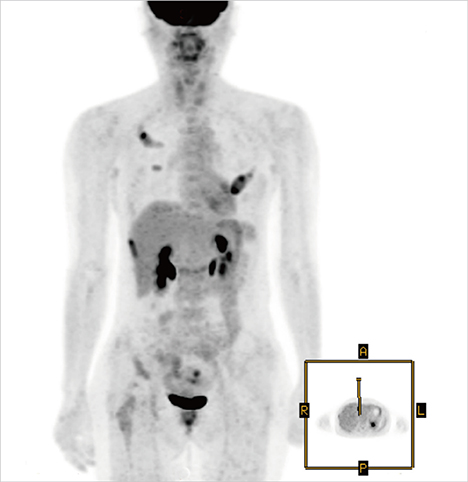
Figure 6 Follow-up 18F-fluorodeoxyglucose (FDG) positron emission tomographic/computed tomographic scan after 1.5 years. Increased FDG uptake in the right first, second, third, eighth, and left fourth ribs, right femur, right ischium, and right ilium, which is suggestive of polyostotic fibrous dysplasia, but which cannot exclude multiple metastases.
Reference
-
1. MacDonald-Jankowski D. Fibrous dysplasia: a systematic review. Dentomaxillofac Radiol. 2009; 38:196–215.
Article2. Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman E, Spiegel AM. Activating mutations of the stimulatory G protein in the McCune-Albright syndrome. N Engl J Med. 1991; 325:1688–1695.
Article3. Zhang Y, Zhao C, Liu H, Hou H, Zhang H. Multiple metastasis-like bone lesions in scintigraphic imaging. J Biomed Biotechnol. 2012; 2012:957364.
Article4. Shigesawa T, Sugawara Y, Shinohara I, Fujii T, Mochizuki T, Morishige I. Bone metastasis detected by FDG PET in a patient with breast cancer and fibrous dysplasia. Clin Nucl Med. 2005; 30:571–573.
Article5. Theriault RL, Carlson RW, Allred C, Anderson BO, Burstein HJ, Edge SB, et al. Breast cancer, version 3. 2013: featured updates to the NCCN guidelines. J Natl Compr Canc Netw. 2013; 11:753–760.6. Lee YT. Bone scanning in patients with early breast carcinoma: should it be a routine staging procedure? Cancer. 1981; 47:486–495.
Article7. Moon DH, Maddahi J, Silverman DH, Glaspy JA, Phelps ME, Hoh CK. Accuracy of whole-body fluorine-18-FDG PET for the detection of recurrent or metastatic breast carcinoma. J Nucl Med. 1998; 39:431–435.8. Choi YJ, Shin YD, Kang YH, Lee MS, Lee MK, Cho BS, et al. The effects of preoperative (18)F-FDG PET/CT in breast cancer patients in comparison to the conventional imaging study. J Breast Cancer. 2012; 15:441–448.
Article9. Cook GJ, Houston S, Rubens R, Maisey MN, Fogelman I. Detection of bone metastases in breast cancer by 18FDG PET: differing metabolic activity in osteoblastic and osteolytic lesions. J Clin Oncol. 1998; 16:3375–3379.
Article10. Wang K, Allen L, Fung E, Chan CC, Chan JC, Griffith JF. Bone scintigraphy in common tumors with osteolytic components. Clin Nucl Med. 2005; 30:655–671.
Article11. Leffler SG, Chew FS. CT-guided percutaneous biopsy of sclerotic bone lesions: diagnostic yield and accuracy. AJR Am J Roentgenol. 1999; 172:1389–1392.
Article12. Han J, Ryu JS, Shin MJ, Kang GH, Lee HK. Fibrous dysplasia with barely increased uptake on bone scan: a case report. Clin Nucl Med. 2000; 25:785–788.13. Lustig LR, Holliday MJ, McCarthy EF, Nager GT. Fibrous dysplasia involving the skull base and temporal bone. Arch Otolaryngol Head Neck Surg. 2001; 127:1239–1247.
Article14. Jones DN, Marion M. Polyostotic fibrous dysplasia as a mimic of bony metastatic disease. Clin Nucl Med. 1991; 16:55–57.
Article15. Roses RE, Arun BK, Lari SA, Mittendorf EA, Lucci A, Hunt KK, et al. Ductal carcinoma-in-situ of the breast with subsequent distant metastasis and death. Ann Surg Oncol. 2011; 18:2873–2878.
Article
