Borrmann Type 4 Advanced Gastric Cancer: Focus on the Development of Scirrhous Gastric Cancer
- Affiliations
-
- 1Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea. mipark@kosinmed.or.kr
- KMID: 2348251
- DOI: http://doi.org/10.5946/ce.2016.057
Abstract
- Early diagnosis of Borrmann type 4 advanced gastric cancer (AGC) is very important for improving the prognosis of AGC patients. Because there is no definite mass in most cases of Borrmann type 4 AGC, its accurate diagnosis via endoscopy requires an understanding of its pathogenesis and developmental process. Moreover, many people confuse linitis plastica (LP) type gastric cancer (GC), scirrhous GC, and Borrmann type 4 AGC. To distinguish each of these cancers, knowledge of their endoscopic and pathological differences is necessary, especially for LP type GCs in the developmental stage. In conclusion, diagnosis of pre-stage or latent LP type GC before progression to typical LP type GC requires the detection of IIc-like lesions in the fundic gland area. It is also crucial to identify any abnormalities such as sclerosis of the gastric wall and hypertrophy of the mucosal folds during endoscopy.
MeSH Terms
Figure
-
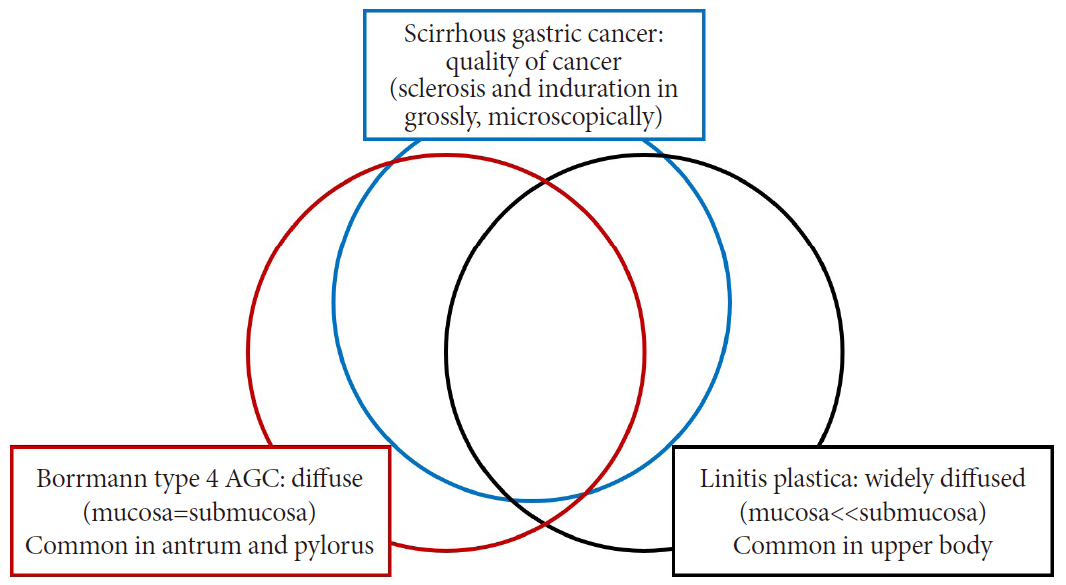
Fig. 1. Relationship between diffuse gastric cancers (scirrhous gastric cancer, Borrmann type 4 advanced gastric cancer [AGC], and linitis plastica).

Fig. 2. Typical case of Borrmann type 4 advanced gastric cancer. These images show similar findings with each diagnostic modality (A, B: endoscopy; C: positron emission tomography-computed tomography [CT]; D, E: abdominal CT). After total gastrectomy, the gross pathologic finding (F) also shows diffuse wall thickening, similar to that observed on CT.
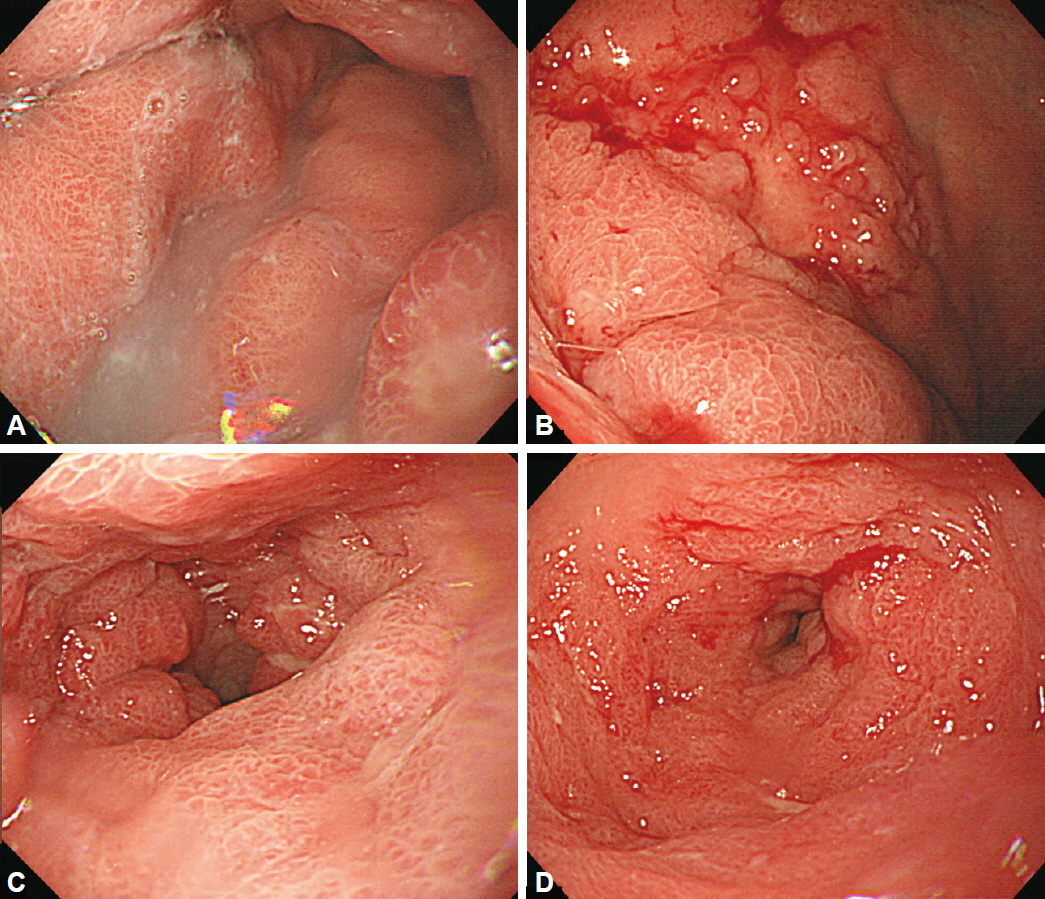
Fig. 3. Examples of scirrhous gastric cancer. (A, B) Diffusely infiltrating masses with local areas of ulceration were present from the body to the distal antrum. (C, D) At the distal antrum, there were wide areas of extensive fibrous hyperplasia and significant luminal narrowing.
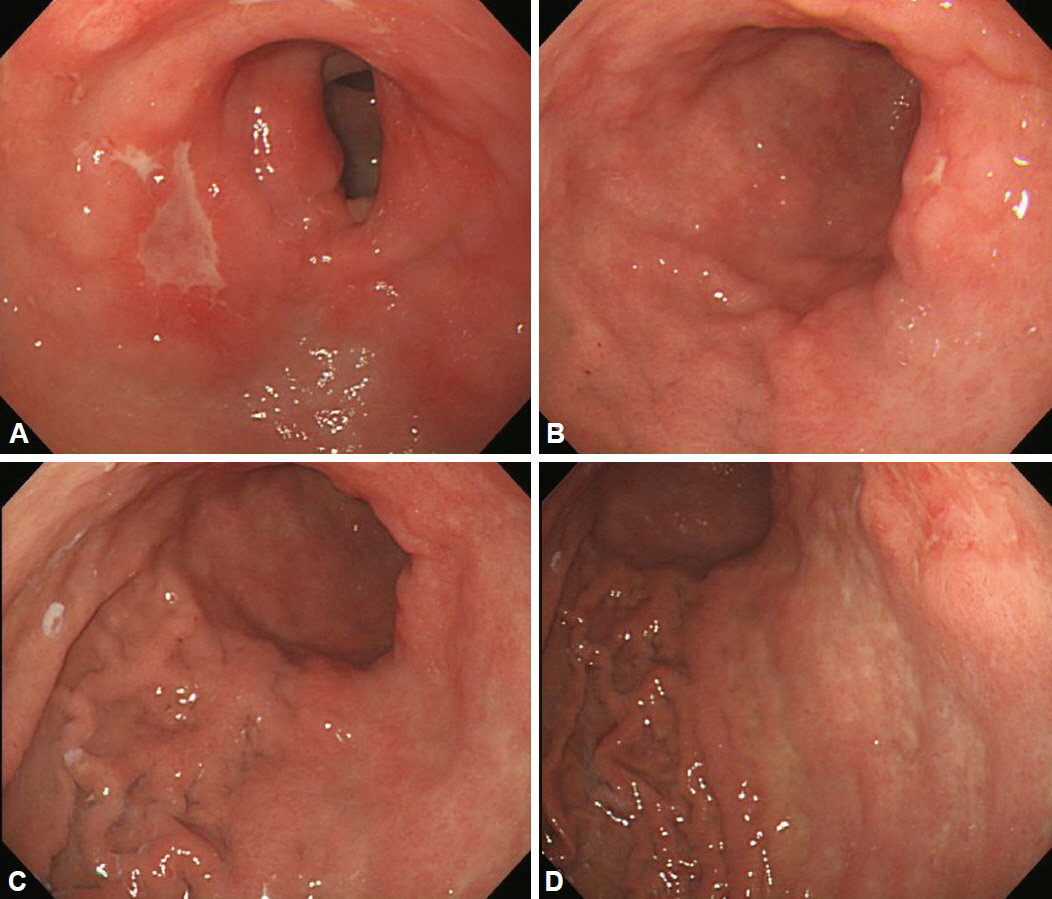
Fig. 4. Examples of Borrmann type 4 advanced gastric cancer. (A, B) At the lesser curvature side of the proximal antrum to the lower body, diffuse, irregular, focal ulceration was observed. (C, D) Diffuse wall thickening and hypertrophy of the mucosal folds were present from the upper body to the antrum, with good distensibility.
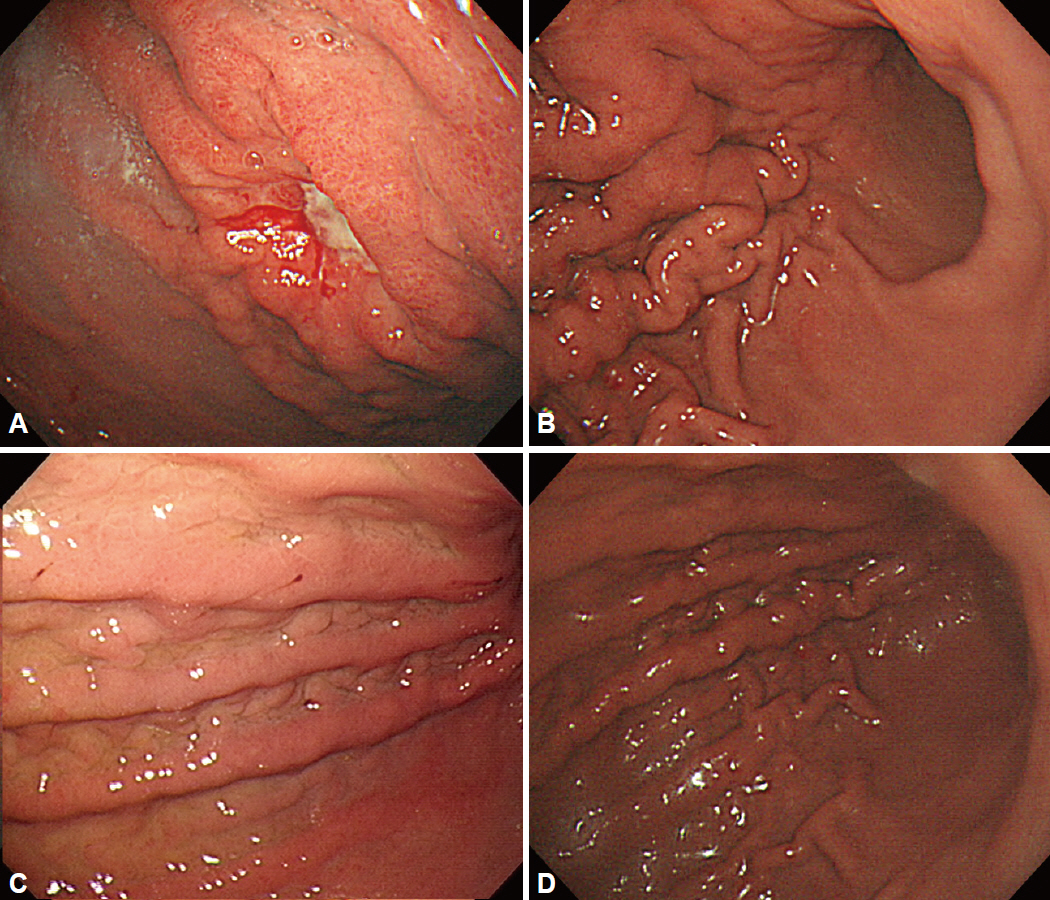
Fig. 5. Examples of linitis plastica gastric cancer. (A, B) There was an ulcerative lesion on the greater curvature side of the upper body with sparing of the antrum. (C, D) Fold thickening with distensibility was observed on the upper to lower body.

Fig. 6. Morphologic changes in linitis plastic gastric cancer. Adapted from Nakamura, with permission from Igaku-Shoin Ltd [16].
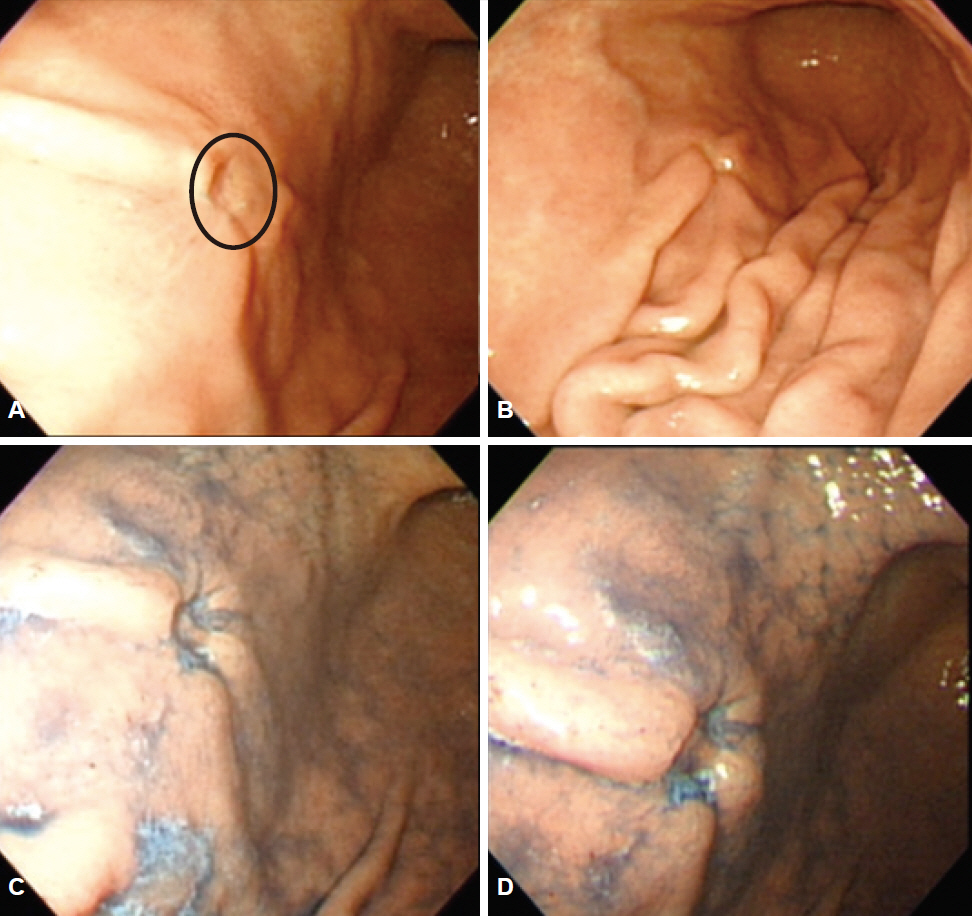
Fig. 7. This picture shows an example of a IIc-like lesion (circle on image A). (A) A 50-year-old man was diagnosed with IIc-type gastric cancer on endoscopic biopsy. (B) Cutting shape of fold convergence was seen on endoscopy. (C, D) After chromoendoscopy with indigo carmine dye, the lesion could be observed more clearly. After gastrectomy, the main lesion was confirmed to be signet ring cell carcinoma without submucosal invasion.
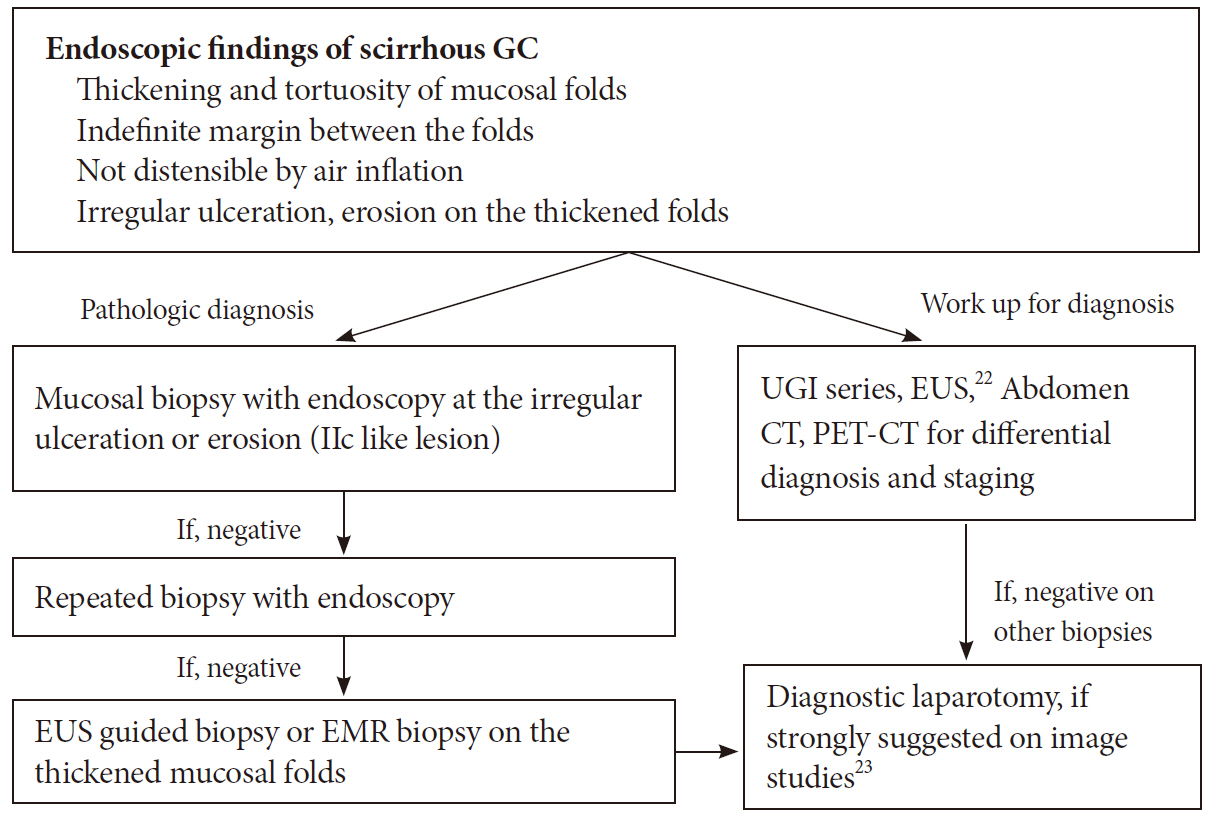
Fig. 8. Summary of endoscopic findings and proposed diagnostic steps for scirrhous gastric cancer (GC). UGI, upper gastrointestinal; EUS, endoscopic ultrasound; CT, computed tomography; PET-CT, positron emission tomography-computed tomography; EMR, endoscopic mucosal resection.
Reference
-
1. Kitamura K, Beppu R, Anai H, et al. Clinicopathologic study of patients with Borrmann type IV gastric carcinoma. J Surg Oncol. 1995; 58:112–117.
Article2. Shim CS. Easy to miss gastric cancer: Borrmann type 4. Paper presented at: The 19th Seminar of Korean Society of Gastrointestinal Endoscopy. 1998 Aug 30-Sep 3; Seoul, Korea.3. Nishi M, Ichikawa H, Nakajima T, Maruyama K, Tahara E. Gastric Cancer. Tokyo: Springer;1993.4. Borrmann R. Geschwülste des Magens und Duodenums. In : Borchardt H, Borrmann R, Christeller E, editors. Verdauungsschlauch: Erster Teil Rachen und Tonsillen, Speiseröhre Magen und Darm, Bauchfell. Vienna: Springer;1926. p. 812–1054.5. Fuchigami T. Historical changes in gastric cancer: from the viewpoint of diagnosis. Stomach Intest. 2005; 40:11–17.6. Park MI. The development of Linitis plastic gastric cancer and similar lesions. Paper presented at: The 13th Seminar of Korean Society of Gastrointestinal Endoscopy. 2006 Jul 9; Busan, Korea.7. Brinton W; Harvard Medical School. Lectures on the Diseases of the Stomach: with an Introduction on Its Anatomy and Physiology. 2nd ed. Philadelphia (PA): Lea and Blanchard;1865.8. Lee JH. Hypertrophic gastritis and Borrmann type IV. Korean J Gastrointest Endosc. 2010; 40(Suppl 1):S83–S85.9. Lee DH. Early endoscopic finding of Borrmann type IV. Korean J Gastrointest Endosc. 2005; 30(Suppl 1):S81–S86.10. Sugiyama N, Baba Y, Takagi K, Nakamura K. A study of the clinical course of linitis plastica type cancer of the stomach: comparison between the clinical course and the development curve of gastric cancer. Stomach Intest. 1980; 15:1153–1163.11. Nakamura K, Kato Y, Misono T, et al. Growing process to carcinoma of linitis plastica type of the stomach from cancer-development. Stomach Intest. 1980; 15:225–234.12. Nakazawa S, Kawaguchi S, Yoshino J, et al. Linitis plastica retrospective study for early detection. Stomach Intest. 1980; 15:1145–1151.13. Takeda S, Suto Y, Kohli Y, et al. Initial findings and developments of linitis plastica type of gastric cancer. Stomach Intest. 1980; 15:1137–1144.14. Ohgushi H, Yao T, Iwashita A. The primary foci of linitis plastics type of gastric cancer and their chronological changes. Stomach Intest. 1980; 15:1129–1136.15. Takizawa T. Distinctive features of linitis plastica type gastric carcinoma with reference to lymphangiosis carcinomatosa. Stomach Intest. 1992; 27:591–598.16. Nakamura K. Issues focused on the IIc lesion in adenocarcima of fundic gland area: from the landscape of “a way to linitis plastica”. Stomach Intest. 1987; 22:999–1001.17. Shim CS. Medical approch for early stomach cancer detection. Paper presented at: Spring Symposim of Cancer of Seoul St. Mary’s Hospital of The Catholic University of Korea. 1996; Seoul, Korea.18. Pedrazzani C, Marrelli D, Pacelli F, et al. Gastric linitis plastica: which role for surgical resection? Gastric Cancer. 2012; 15:56–60.
Article19. Hosokawa O, Kaizaki Y, Miyanaga T, et al. Endoscopic study of the early phase in linitis plastica type gastric gancer. Stomach Intest. 2008; 43:799–809.20. Maruyama Y, Kageoka M, Nagata K, et al. Endoscopic diagnosis based on typical findings of scirrhous gastric cancer. Stomach Intest. 2010; 45:445–455.21. Jeong HY. AGC Borrmann type IV cancer. Korean J Gastrointest Endosc. 2011; 43(Suppl 2):S215–S217.22. Kim JO, Ryu CB, Cho JY, Lee JS, Lee MS, Shim CS. The usefulness of the endoscopic ultrasonography in the evaluation of the thickened gastric wall. Korean J Gastrointest Endosc. 2001; 22:139–145.23. Ahn JB, Ha TK, Lee HR, Kwon SJ. An insufficient preoperative diagnosis of Borrmann type 4 gastric cancer in spite of EMR. J Gastric Cancer. 2011; 11:59–63.
Article24. Levine MS, Kong V, Rubesin SE, Laufer I, Herlinger H. Scirrhous carcinoma of the stomach: radiologic and endoscopic diagnosis. Radiology. 1990; 175:151–154.
Article25. Murata Y, Yamasaki T, Kitamura Y, et al. Diagnostic points of endoscopic ultrasonographic findings in scirrhous gastric cancer. Stomach Intest. 2010; 45:457–467.26. Songür Y, Okai T, Watanabe H, Motoo Y, Sawabu N. Endosonographic evaluation of giant gastric folds. Gastrointest Endosc. 1995; 41:468–474.
Article27. Roh M, Sohn JH, Kim TY, et al. Gastric syphilis and membranous glomerulonephritis. Clin Endosc. 2015; 48:256–259.
Article28. Kamijo Y, Kondo I, Watanabe M, Kan’o T, Ide A, Soma K. Gastric stenosis in severe corrosive gastritis: prognostic evaluation by endoscopic ultrasonography. Clin Toxicol (Phila). 2007; 45:284–286.
Article29. Jee SR. Borrmann type 4 AGC. Paper presented at: The 46th Korean Society of Gastrointestinal Endoscopy Seminar. 2012 Mar 25; Goyang, Korea.30. Chung IS, Park DH, Choi SW, et al. Esophagus, stomach & intestine: a case of Menetrier’s disease. Korean J Gastrointest Endosc. 1997; 17:167–172.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcome of Surgical Treatment for Borrmann Type 4 Gastric Cancer
- Clinicopathological Features of Borrmann Type IV Gastric Carcinomas
- Clinicopathological Analysis of Borrmann Type IV Gastric Cancer
- Endoscopic Findings and Its Diagnostic Accuracy in Gastric Cancer Confirmed by Surgery
- Two Cases of Huge Polypoid Early Gastric Cancer
