Cancer Res Treat.
2005 Apr;37(2):87-91.
Clinicopathological Analysis of Borrmann Type IV Gastric Cancer
- Affiliations
-
- 1Department of Surgery, Ulsan University College of Medicine, Seoul, Korea. jhyook@amc.seoul.kr
Abstract
- PURPOSE
Borrmann type IV gastric cancer is often diagnosed only at an advanced stage, resulting in a prognosis poor. We performed a retrospective study of the clinical characteristics of Borrmann type IV gastric cancer and the prognostic factors affecting the survival rate in such patients. MATERIALS AND METHODS: Of 4, 063 patients with all gastric cancers, 370 (9%) with Borrmann type IV gastric cancer were analyzed. RESULTS: The clinical characteristics of these patients included a higher incidence rate in young females, and higher rates of serosa exposure, metastasis to lymph nodes and early peritoneal dissemination. Of patients presenting with peritoneal seeding, those resected had a higher survival rate than those that were not. A univariate analysis showed that the prognostic factors affecting the survival rate following a curative resection were the location, occupied area and depth of the primary tumor, as well as the presence of lymph node metastasis and the tumor stage. A multivariate analysis indicated that the tumor location and stage were significant independent prognostic factors after a curative resection for Borrmann type IV gastric cancer. CONCLUSION: In conclusion, the early diagnosis and treatment of patients with Borrmann type IV gastric cancer are essential for the better survival of these patients. Even in patients with advanced tumors, a noncurative palliative resection may improve the prognosis.
Keyword
MeSH Terms
Figure
-
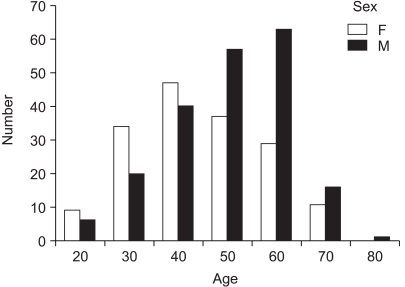
Fig. 1 Age and sex distribution.

Fig. 2 Comparison of survival rate between curative resection and other group (p<0.05).
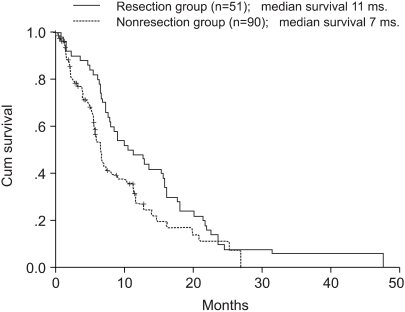
Fig. 3 Comparison of survival rate between resection and nonresection group in peritoneal seeding patients (p<0.05).
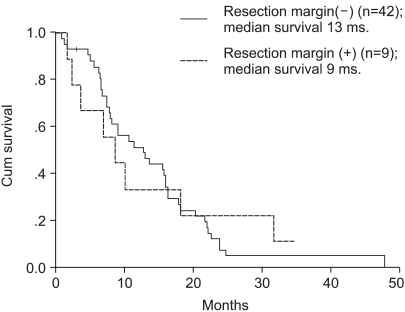
Fig. 4 Comparison of effect to survival rate between negative and positive resection margin of gastrectomy in peritoneal seeding patients (p=0.84).
Reference
-
1. Kitamura K, Beppu R, Anai H, Ikejiri K, Yakabe S, Sugimachi K, et al. Clinicopathologic study of patients with Borrmann type IV gastric carcinoma. J Surg Oncol. 1995; 58:112–117. PMID: 7844980.
Article2. Maehara Y, Moriguchi S, Orita H, Kakeji Y, Haraguchi M, Korenaga D, et al. Lower survival rate for patients with carcinoma of the stomach of Borrmann type IV after gastric section. Surg Gynecol Obstet. 1992; 175:13–16. PMID: 1621194.3. Moriguchi S, Maehara Y, Korenaga D, Sugimachi K, Nose Y. Risk factors which predict pattern of recurrence after curative surgery for patients with advanced gastric cancer. Surg Oncol. 1992; 1:341–346. PMID: 1341269.
Article4. Japanese Research Society for Gastric Cancer. Japanese classification of gastric carcinoma. 1998. 2nd English ed. Tokyo: Kanehara.5. Hirose S, Honjou H, Nakagawa H, Nishimura K, Kuroda Y, Tsuji M, et al. Scirrhous carcinoma of the stomach: a clinical and pathological study of 106 surgical cases. Gastroenterol Jpn. 1989; 24:481–487. PMID: 2553523.
Article6. Nagayo T, Yokoyama H. Scirrhous carcinoma occurring in the corpus (body) of the stomach. Acta Pathol Jpn. 1974; 24:797–814. PMID: 4376327.
Article7. Sugano H, Nakamura K, Kato Y. Pathological studies of human gastric cancer. Acta Pathol Jpn. 1982; 32(suppl 2):329–347. PMID: 6765003.8. Kim JP, Lee JH, Kim SJ, Yu HJ, Yang HK. Clinicopathologic characteristics and prognostic factors in 10,783 patients with gastric cancer. Gastric Cancer. 1998; 1:125–133. PMID: 11957056.9. Kinugasa S, Abe S, Tachibana M, Yoshimura H, Monden N, Dhar DK, et al. Surgically curable and incurable scirrhous carcinomas of the stomach. J Surg Oncol. 1997; 65:194–200. PMID: 9236929.
Article10. Aranha GV, Georgen R. Gastric linitis plastica is not a surgical disease. Surgery. 1989; 106:758–762. PMID: 2552599.11. Furukawa H, Hiratsuka M, Iwanaga T, Imaoka S, Ishikawa O, Kabuto T, et al. Extended surgery-left upper abdominal exenteration plus Appleby's method-for type 4 gastric carcinoma. Ann Surg Oncol. 1997; 4:209–214. PMID: 9142381.
Article12. Otsuji E, Yamaguchi T, Sawai K, Sakakura C, Okamoto K, Takahashi T. Regional lymph node metastasis as a predictor of peritoneal carcinomatosis in patients with Borrmann type IV gastric carcinoma. Am J Gastroenterol. 1999; 4:434–437. PMID: 10022642.
Article13. Furukawa H, Hiratsuka M, Iwanaga T. A rational technique for surgical operation on Borrmann type 4 gastric carcinoma: left upper abdominal evisceration plus Appleby's method. Br J Surg. 1988; 75:116–119. PMID: 3349295.
Article14. Arveux P, Faivre J, Boutron MC, Piard F, Dusserre-Guion L, Monnet E, et al. Prognosis of gastric carcinoma after curative surgery. A population-based study using multivariate crude and relative survival analysis. Dig Dis Sci. 1992; 37:757–763. PMID: 1563320.15. Hanazaki K, Sodeyama H, Mochizuki Y, Igarashi J, Yokoyama S, Sode Y, et al. Palliative gastrectomy for advanced gastric cancer. Hepatogastroenterology. 2001; 48:285–289. PMID: 11268986.16. Maeta M, Sugesawa A, Ikeguchi M, Tsujitani S, Yamashiro H, Shibata S, et al. Does the extent of lymph node dissection affect the postoperative survival of patients with gastric cancer and disseminating peritoneal metastases? Surg Today. 1994; 24:40–43. PMID: 7519911.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinicopathological Features of Borrmann Type IV Gastric Carcinomas
- Clinicopathologic Characteristics of and Prognosis for Patients with a Borrmann Type IV Gastric Carcinoma
- Outcome of Surgical Treatment for Borrmann Type 4 Gastric Cancer
- Clinicopathologic Characteristics of Borrmann Type 4 Gastric Cancer
- Clinicopathologic Characteristics and Prognostic Factors of Long-term Survivors of Borrmann Type 4 Gastric Cancer
