J Korean Med Sci.
2015 Oct;30(10):1459-1465. 10.3346/jkms.2015.30.10.1459.
The Prognostic Value of Residual Volume/Total Lung Capacity in Patients with Chronic Obstructive Pulmonary Disease
- Shin TR

- Oh YM
- Park JH
- Lee KS
- Oh S
- Kang DR
- Sheen S
- Seo JB
- Yoo KH
- Lee JH
- Kim TH
- Lim SY
- Yoon HI
- Rhee CK
- Choe KH
- Lee JS
- Lee SD
- Affiliations
-
- 1Division of Pulmonology, Allergy & Critical Care Medicine, Department of Internal Medicine, Hallym University Medical Center, Seoul, Korea.
- 2Department of Pulmonary and Critical Care Medicine and Clinical Research Center for Chronic Obstructive Airway Diseases, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Pulmonary and Critical Care Medicine, Ajou University School of Medicine, Suwon, Korea. jhpamc@hanmail.net
- 4Office of Biostatistics, Medical Humanities and Social Medicine, Ajou University School of Medicine, Seoul, Korea.
- 5Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 6Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea.
- 7Department of Internal Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 8Division of Pulmonology, Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
- 9Division of Pulmonary and Critical Care Medicine, Department of Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 10Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 11Department of Internal Medicine, Seoul St. Mary's Hospital, Catholic University of Korea, Seoul, Korea.
- 12Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, College of Medicine, Chungbuk National University, Cheongju, Korea.
- KMID: 2344179
- DOI: http://doi.org/10.3346/jkms.2015.30.10.1459
Abstract
- The prognostic role of resting pulmonary hyperinflation as measured by residual volume (RV)/total lung capacity (TLC) in chronic obstructive pulmonary disease (COPD) remains poorly understood. Therefore, this study aimed to identify the factors related to resting pulmonary hyperinflation in COPD and to determine whether resting pulmonary hyperinflation is a prognostic factor in COPD. In total, 353 patients with COPD in the Korean Obstructive Lung Disease cohort recruited from 16 hospitals were enrolled. Resting pulmonary hyperinflation was defined as RV/TLC > or = 40%. Multivariate logistic regression analysis demonstrated that older age (P = 0.001), lower forced expiratory volume in 1 second (FEV1) (P < 0.001), higher St. George Respiratory Questionnaire (SGRQ) score (P = 0.019), and higher emphysema index (P = 0.010) were associated independently with resting hyperinflation. Multivariate Cox regression model that included age, gender, dyspnea scale, SGRQ, RV/TLC, and 6-min walking distance revealed that an older age (HR = 1.07, P = 0.027), a higher RV/TLC (HR = 1.04, P = 0.025), and a shorter 6-min walking distance (HR = 0.99, P < 0.001) were independent predictors of all-cause mortality. Our data showed that older age, higher emphysema index, higher SGRQ score, and lower FEV1 were associated independently with resting pulmonary hyperinflation in COPD. RV/TLC is an independent risk factor for all-cause mortality in COPD.
Keyword
MeSH Terms
-
Aged
Dyspnea/diagnosis/physiopathology
Exercise Test
Exercise Tolerance
Female
Forced Expiratory Flow Rates/physiology
Forced Expiratory Volume
Humans
Lung/*physiopathology
Male
Middle Aged
Prognosis
Pulmonary Disease, Chronic Obstructive/*diagnosis/mortality/physiopathology
Pulmonary Emphysema/*diagnosis/mortality/physiopathology
Republic of Korea
Residual Volume/*physiology
Respiratory Function Tests
Surveys and Questionnaires
Total Lung Capacity/*physiology
Vital Capacity
Walking/physiology
Figure
-

Fig. 1 Flow diagram of the subjects who were enrolled in this study.
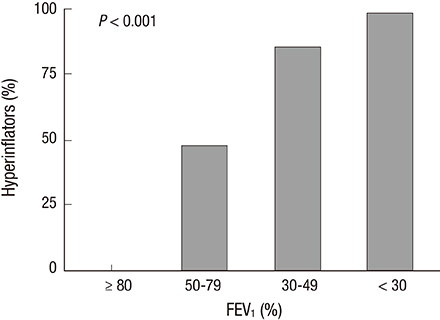
Fig. 2 Rate of hyperinflators (RV/TLC ≥ 40%) according to FEV1.

Fig. 3 Rate of frequent exacerbations according to RV/TLC. Frequency of frequent exacerbations in (A) the year before enrollment and (B) during the first year of follow-up. RV/TLC, residual volume/total lung capacity.
Reference
-
1. Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013; 187:347–365.2. Ferguson GT. Why does the lung hyperinflate? Proc Am Thorac Soc. 2006; 3:176–179.3. Casanova C, Cote C, de Torres JP, Aguirre-Jaime A, Marin JM, Pinto-Plata V, Celli BR. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005; 171:591–597.4. Martinez FJ, de Oca MM, Whyte RI, Stetz J, Gay SE, Celli BR. Lung-volume reduction improves dyspnea, dynamic hyperinflation, and respiratory muscle function. Am J Respir Crit Care Med. 1997; 155:1984–1990.5. Marchand E, Gayan-Ramirez G, De Leyn P, Decramer M. Physiological basis of improvement after lung volume reduction surgery for severe emphysema: where are we? Eur Respir J. 1999; 13:686–696.6. Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002; 121:1434–1440.7. Budweiser S, Harlacher M, Pfeifer M, Jörres RA. Co-morbidities and hyperinflation are independent risk factors of all-cause mortality in very severe COPD. COPD. 2014; 11:388–400.8. Slebos DJ, Klooster K, Ernst A, Herth FJ, Kerstjens HA. Bronchoscopic lung volume reduction coil treatment of patients with severe heterogeneous emphysema. Chest. 2012; 142:574–582.9. Lahaije AJ, van Helvoort HA, Dekhuijzen PN, Vercoulen JH, Heijdra YF. Resting and ADL-induced dynamic hyperinflation explain physical inactivity in COPD better than FEV1. Respir Med. 2013; 107:834–840.10. Krieger BP. Hyperinflation and intrinsic positive end-expiratory pressure: less room to breathe. Respiration. 2009; 77:344–350.11. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995; 152:1107–1136.12. Albuquerque AL, Nery LE, Villaça DS, Machado TY, Oliveira CC, Paes AT, Neder JA. Inspiratory fraction and exercise impairment in COPD patients GOLD stages II-III. Eur Respir J. 2006; 28:939–944.13. Wouters EF, Postma DS, Fokkens B, Hop WC, Prins J, Kuipers AF, Pasma HR, Hensing CA, Creutzberg EC. COSMIC (COPD and Seretide: a Multi-Center Intervention and Characterization) Study Group. Withdrawal of fluticasone propionate from combined salmeterol/fluticasone treatment in patients with COPD causes immediate and sustained disease deterioration: a randomised controlled trial. Thorax. 2005; 60:480–487.14. Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007; 370:786–796.15. Gevenois PA, de Maertelaer V, De Vuyst P, Zanen J, Yernault JC. Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med. 1995; 152:653–657.16. Wood SA, Zerhouni EA, Hoford JD, Hoffman EA, Mitzner W. Measurement of three-dimensional lung tree structures by using computed tomography. J Appl Physiol. 1995; 79:1687–1697.17. Lee YK, Oh YM, Lee JH, Kim EK, Lee JH, Kim N, Seo JB, Lee SD. KOLD Study Group. Quantitative assessment of emphysema, air trapping, and airway thickening on computed tomography. Lung. 2008; 186:157–165.18. Nakano Y, Muro S, Sakai H, Hirai T, Chin K, Tsukino M, Nishimura K, Itoh H, Paré PD, Hogg JC, et al. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function. Am J Respir Crit Care Med. 2000; 162:1102–1108.19. O'Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001; 164:770–777.20. Tantucci C, Duguet A, Similowski T, Zelter M, Derenne JP, Milic-Emili J. Effect of salbutamol on dynamic hyperinflation in chronic obstructive pulmonary disease patients. Eur Respir J. 1998; 12:799–804.21. Marin JM, Carrizo SJ, Gascon M, Sanchez A, Gallego B, Celli BR. Inspiratory capacity, dynamic hyperinflation, breathlessness, and exercise performance during the 6-minute-walk test in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001; 163:1395–1399.22. Diaz O, Villafranca C, Ghezzo H, Borzone G, Leiva A, Milic-Emil J, Lisboa C. Role of inspiratory capacity on exercise tolerance in COPD patients with and without tidal expiratory flow limitation at rest. Eur Respir J. 2000; 16:269–275.23. O'Donnell DE, Webb KA. Exertional breathlessness in patients with chronic airflow limitation. The role of lung hyperinflation. Am Rev Respir Dis. 1993; 148:1351–1357.24. Nishimura K, Yasui M, Nishimura T, Oga T. Airflow limitation or static hyperinflation: which is more closely related to dyspnea with activities of daily living in patients with COPD? Respir Res. 2011; 12:135.25. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease. Revised 2011. accessed on 15 July 2015. Available at http://www.goldcopd.org/uploads/users/files/GOLD_Report_2011_Feb21.pdf.26. Domingo-Salvany A, Lamarca R, Ferrer M, Garcia-Aymerich J, Alonso J, Félez M, Khalaf A, Marrades RM, Monsó E, Serra-Batlles J, et al. Health-related quality of life and mortality in male patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002; 166:680–685.27. Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, Pinto Plata V, Cabral HJ. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004; 350:1005–1012.28. Hurst JR, Vestbo J, Anzueto A, Locantore N, Müllerova H, Tal-Singer R, Miller B, Lomas DA, Agusti A, Macnee W, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010; 363:1128–1138.29. O'Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006; 3:180–184.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Differences in Resting Pulmonary Function in Relation to the Nutritional status of Patients with Chronic Obstructive Pulmonary Disease
- Correlation between Caloric Intake and Lung Function Parameters in Patients with Chronic Obstructive Pulmonary Disease
- Diagnosis of chronic obstructive pulmonary disease
- Beyond the Spirometry: New Diagnostic Modalities in Chronic Obstructive Pulmonary Disease
- Partial Flow Volume Curve in Patients with Obstructive Ventilatory Disorder
