Isolated Oculomotor Nerve Palsy due to Direct Invasion of Recurrent Diffuse Large B-Cell Lymphoma
- Affiliations
-
- 1Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Ophthalmology, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea. khyeye@paran.com
Abstract
- PURPOSE
Compared with multiple cranial nerve palsies, isolated nerve palsy is very rare in Non-Hodgkin's lymphoma. We experienced a case of isolated oculomotor nerve palsy as the first sign of recurrent diffuse large B-cell lymphoma (DLBCL).
CASE SUMMARY
A 45-year-old woman visited the ophthalmology clinic with a one-month history of left upper eyelid ptosis and diplopia. She had a history of DLBCL of the nasopharynx and has been in complete remission for three years after systemic chemotherapy. Ophthalmologic evaluation showed ptosis of the upper eyelid, anisocoria, but no definite limitations in ocular movement. After six weeks, aggravated ptosis, exodeviation of the left eye in the primary position, and ocular movement limitations in all directions except abduction were observed. Brain magnetic resonance angiography taken four weeks earlier demonstrated no intracranial vascular lesion, but an enhancing lesion in the cistern along the left oculomotor nerve was shown in brain magnetic resonance imaging. We diagnosed isolated oculomotor nerve palsy due to direct invasion of recurrent DLBCL. Cerebrospinal fluid analysis revealed tumor cells, and follow-up MRI showed progression of lymphoma into the cavernous sinus.
CONCLUSIONS
Although not common, isolated oculomotor nerve palsy can be the first sign of malignant lymphoma, even after complete remission.
Keyword
MeSH Terms
-
Anisocoria
B-Lymphocytes
Blepharoptosis
Brain
Caves
Cranial Nerve Diseases
Diplopia
Exotropia
Eye
Eyelids
Female
Follow-Up Studies
Humans
Lymphoma
Lymphoma, B-Cell
Lymphoma, Non-Hodgkin
Magnetic Resonance Angiography
Magnetic Resonance Imaging
Middle Aged
Nasopharynx
Oculomotor Nerve
Oculomotor Nerve Diseases
Ophthalmology
Paralysis
Figure
-

Figure 1 At the initial presentation, left eyelid ptosis is noted, but there was no definite ocular movement limitation.
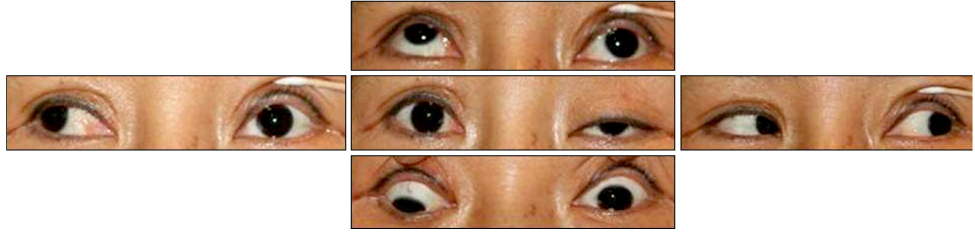
Figure 2 After 6 weeks, left eyelid ptosis is aggravated. Ocular movements were limited in all directions, except abduction.
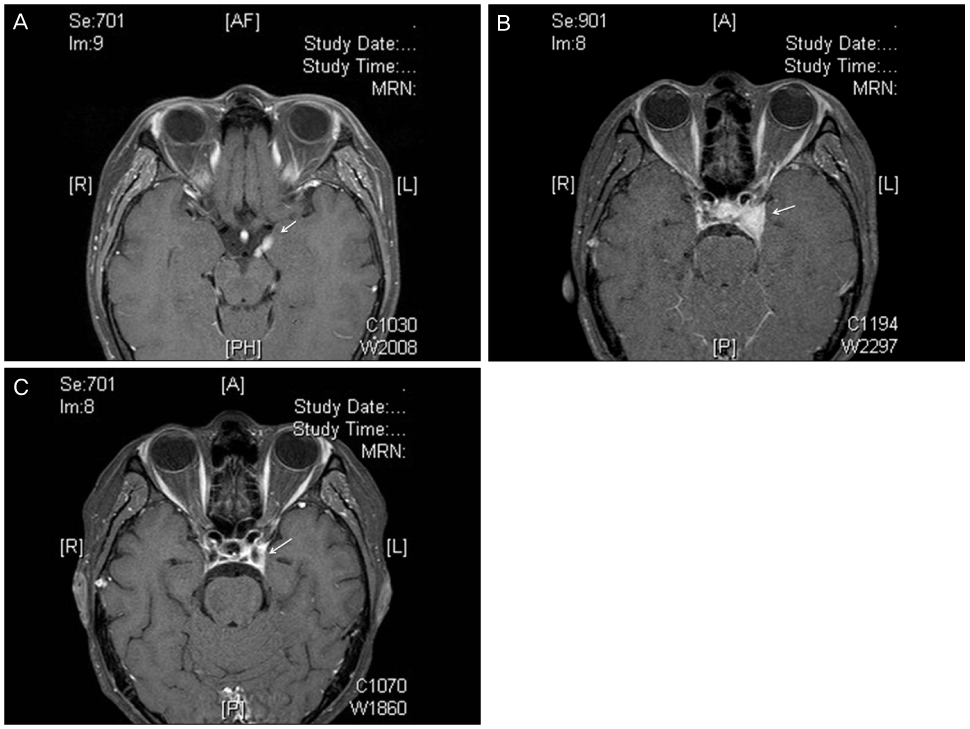
Figure 3 T1-weighted fat suppression with delayed gadolinium enhancement magnetic resonance imaging (MRI) of the brain. (A) MRI 2 weeks after the initial presentation. Enhanced cisternal segment of the oculomotor nerve (arrow) is noted. (B) MRI 6 weeks after initial presentation, right before systemic therapy for recurrent lymphoma. Increased enhanced lesion of in cavernous sinus is marked (arrow). (C) MRI 1 month after systemic therapy demonstrates decreased enhanced lesions in the cavernous sinus (arrow).
Reference
-
1. MacKintosh FR, Colby TV, Podolsky WJ, et al. Central nervous system involvement in non-Hodgkin's lymphoma: an analysis of 105 cases. Cancer. 1982. 49:586–595.2. Levy J, Kratz A, Lifshitz T. Burkitt's lymphoma presenting as oculomotor palsy in an HIV-positive patient. Eur J Ophthalmol. 2006. 16:186–189.3. Keane JR. Cavernous sinus syndrome. Analysis of 151 cases. Arch Neurol. 1996. 53:967–971.4. Kline LB, Hoyt WF. The Tolosa-Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001. 71:577–582.5. Park YM, Cho JH, Cho JY, et al. Non-Hodgkin's lymphoma of the sphenoid sinus presenting as isolated oculomotor nerve palsy. World J Surg Oncol. 2007. 5:86.6. Manabe Y, Kurokawa K, Kashihara K, Abe K. Isolated oculomotor nerve palsy in lymphoma. Neurol Res. 2000. 22:347–348.7. Bhatti MT, Schmalfuss IM, Eskin TA. Isolated cranial nerve III palsy as the presenting manifestation of HIV-related large B-cell lymphoma: clinical, radiological and postmortem observations: report of a case and review of the literature. Surv Ophthalmol. 2005. 50:598–606.8. Kajiya Y, Nakajo M, Kajiya Y, Miyaji N. Oculomotor nerve invasion by lymphoma demonstrated by MRI. J Comput Assist Tomogr. 1995. 19:502–504.9. Choi SM, Kim JT, Lee SH, et al. Isolated oculomotor nerve palsy due to Non-Hodgkin's lymphoma demonstrated by serial MRI. Chonnam Med J. 2008. 44:109–112.10. Brazis PW. Isolated palsies of cranial nerves III, IV and VI. Semin Neurol. 2009. 29:14–28.11. Liang C, Du Y, Lin X, et al. Anatomical features of the cisternal segment of the oculomotor nerve: neurovascular relationships and abnormal compression on magnetic resonance imaging. J Neurosurg. 2009. 111:1193–1200.12. Kan S, Ikeda T. Gd-DTPA enhancement of cranial nerves on MR imaging. Neoplastic lesions. Acta Neurol Scand. 1999. 100:400–406.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Oculomotor Nerve Palsy due to Non-Hodgkin's Lymphoma Demonstrated by Serial MRI
- Isolated Oculomotor Nerve Palsy Caused by Onodi Cell Sinusitis
- Pituitary Apoplexy Presenting as Isolated Oculomotor Nerve Palsy
- A Case of Isolated Complete Oculomotor Nerve Palsy Following Endoscopic Sinus Surgery
- Neurolymphomatosis Involving Antebrachial Cutaneous Nerve
