Brain Abscess Formation Accompanied by Improvement of Orbital Cellulitis
- Affiliations
-
- 1Department of Ophthalmology, Gachon University, Gil Hospital, Incheon, Korea. cmj@gilhospital.com
Abstract
- PURPOSE
To present a case of brain abscess formation accompanied by improvement of orbital cellulitis.
CASE SUMMARY
A 54-year-old male came to our clinic complaining of swelling and pain of the left periorbital area and decreased visual acuity (VA) of the left eye. Initial best-corrected visual acuity (BCVA) was 0.3 and intraocular pressure was 27 mmHg in the left eye. Eye movement in all directions was restricted and 4 mm of proptosis was observed in the left eye. An orbital CT scan demonstrated pansinusitis and orbital cellulitis of the left eye. The patient underwent endoscopic sinus surgery and was treated with systemic antibiotics. However, periorbital swelling was aggravated and another orbital CT scan was performed and analyzed. The CT scan showed localized periorbital abscess of the left eye, and the authors performed an incision and drainage (I&D) of abscess procedure. After the operation, BCVA of the left eye was recovered to 0.8 and eye movement improved and periorbital swelling decreased. However, 15 days after the I&D, the patient complained of a severe headache. Brain magnetic resonance imaging (MRI) was performed and showed an abscess of the left frontal lobe of the brain. The authors consulted with a neurosurgeon, and the patient received intravenous antibiotics and mannitol. The headache steadily decreased, and three months after the first visit, a follow-up brain MRI was performed. The MRI showed almost complete disappearance of the abscess and six months after the first visit, BCVA was recovered to 1.0 and eye movement was full in all directions.
CONCLUSIONS
Although orbital cellulitis is improved by treatment of antibiotics and surgery, if the patient complains of neurologic symptoms such as headache, other complications such as brain abscess formation should be considered.
Keyword
MeSH Terms
-
Abscess
Anti-Bacterial Agents
Brain
Brain Abscess
Drainage
Exophthalmos
Eye
Eye Movements
Follow-Up Studies
Frontal Lobe
Headache
Humans
Intraocular Pressure
Magnetic Resonance Imaging
Male
Mannitol
Middle Aged
Neurologic Manifestations
Orbit
Orbital Cellulitis
Porphyrins
Sinusitis
Visual Acuity
Anti-Bacterial Agents
Mannitol
Porphyrins
Figure
-

Figure 1. Photographs at admission. These photographs demonstrate periorbital swelling, ptosis, exophthalmos and restriction of eye movement in the left eye.
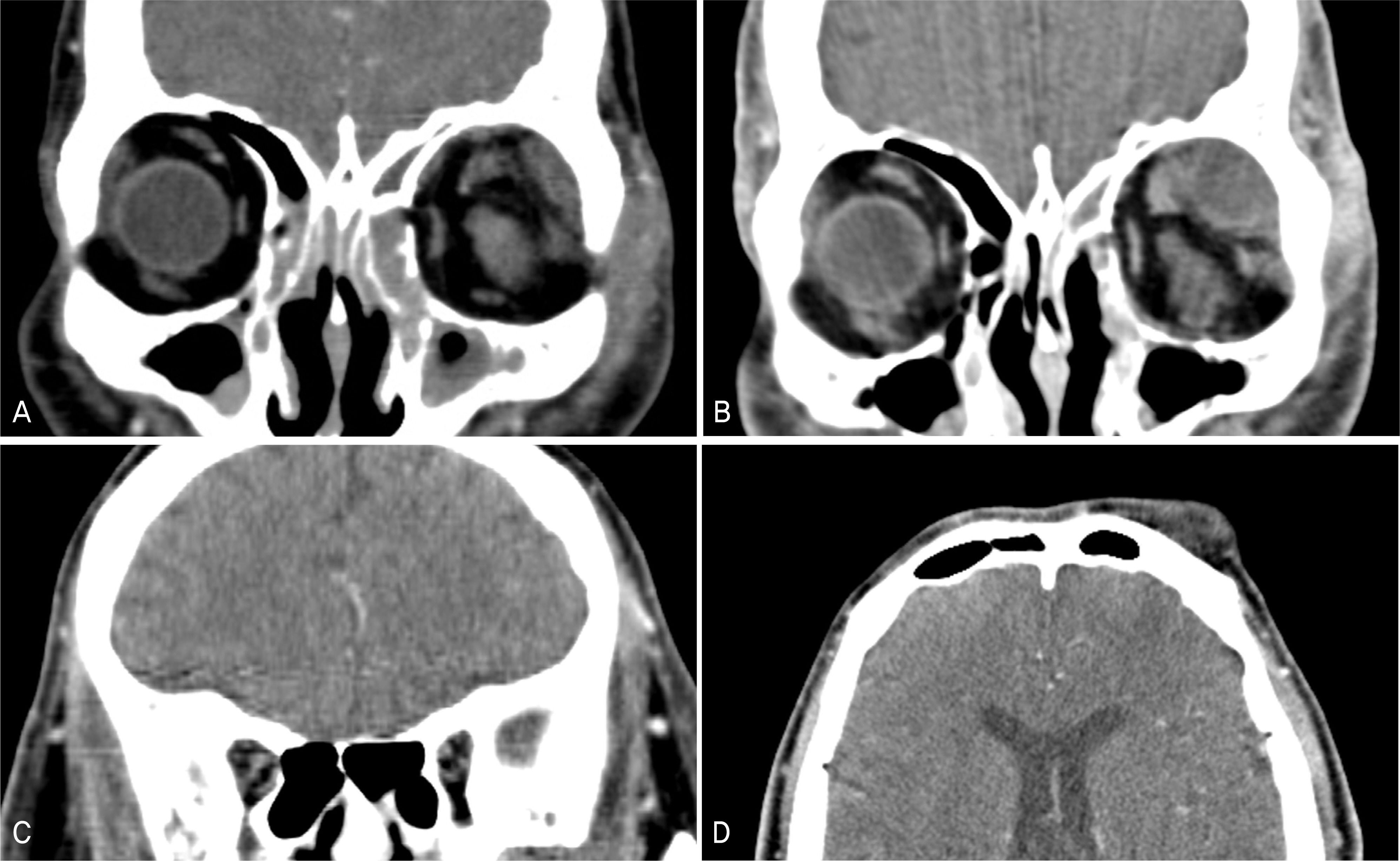
Figure 2. (A) Orbital CT scan at admission. Enhanced soft tissue densities in left orbit and both maxillary sinus, ethmoid, sphenoid, frontal sinus. (B, C, D) Follow up orbital CT scan. Aggravated state of Inflammation in left orbit (abscess formation) and no evidence of intracranial extension of inflammation.
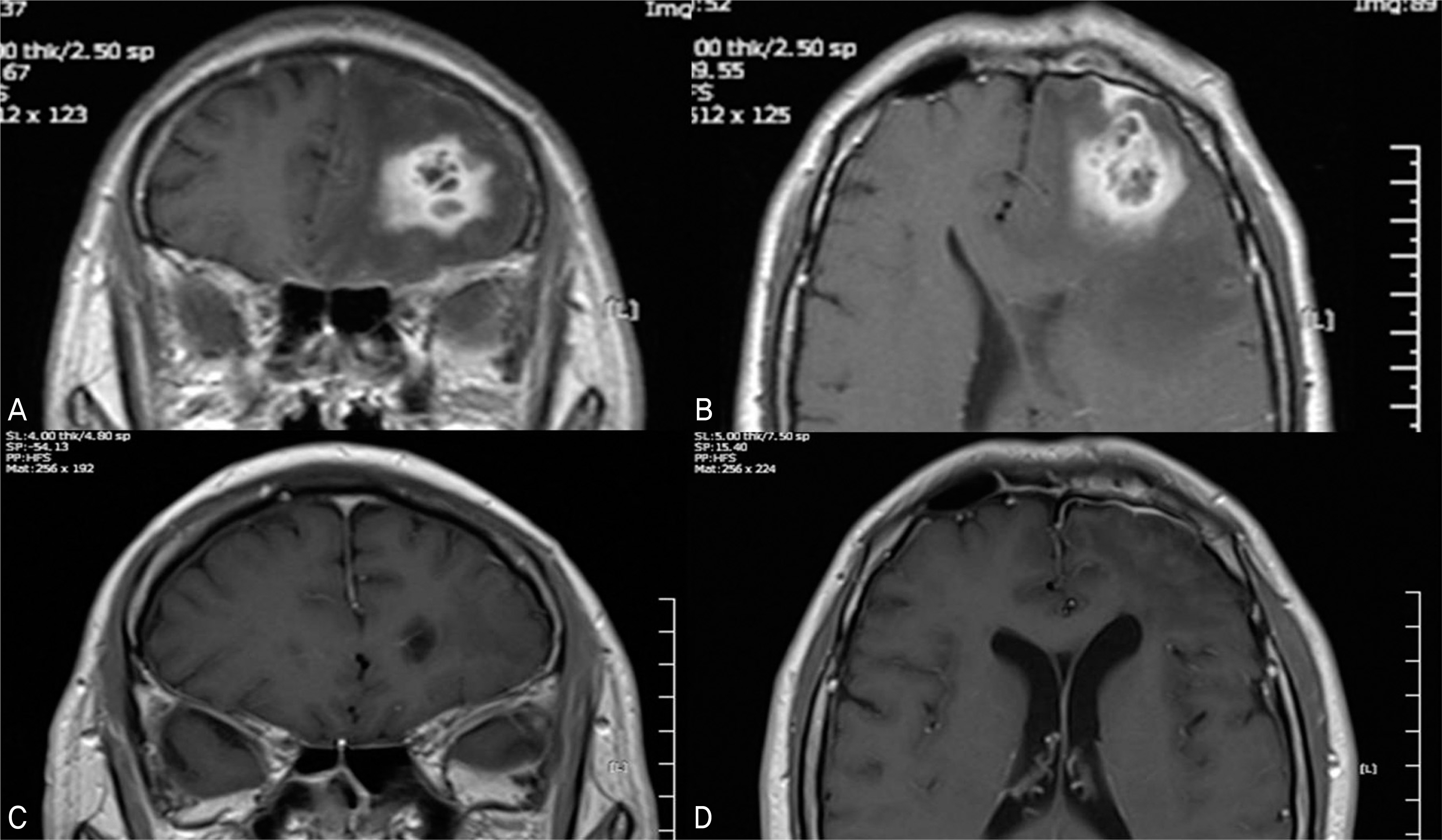
Figure 3. (A, B) T1-weighted MRI scans. Newly developed enhancing multilocular lesion (abscess) and surrounding edema in left forntal lobe. (C, D) Follow up T1-weighted MRI scans. Improved state of brain abscess and atrophic change of left frontal lobe.
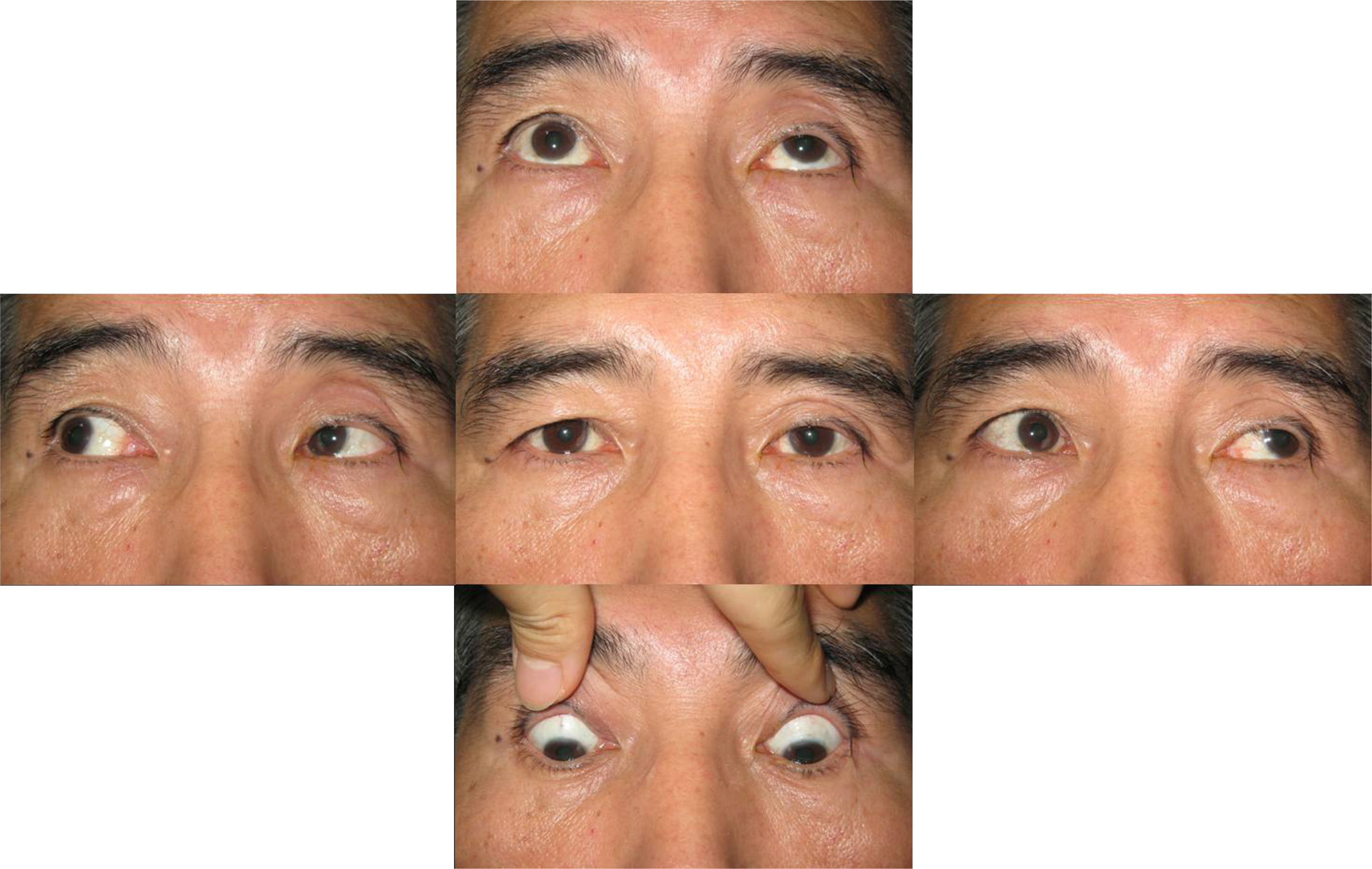
Figure 4. Photographs at final visit. Almost recovered restriction of left eye movement.
Reference
-
References
1. Martin-Hirsch DP, Habashi S, Hinton AH, Kotecha B. Orbital cellulitis. Arch Emerg Med. 1992; 9:143–8.
Article2. Gallagher RM, Gross CW, Phillips CD. Suppurative intracranial complications of sinusitis. Laryngoscope. 1998; 108:1635–42.
Article3. Xiao F, Tseng MY, Teng LJ, et al. Brain abscess: clinical experience and analysis of prognostic factors. Surg Neurol. 2005; 63:442–50.
Article4. Lavania A, Sharma V, Reddy NS, Baksh R. Orbital cellulitis-a complication of sinusitis. Kathmandu Univ Med J. 2005; 3:292–3.5. Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970; 80:1414–28.
Article6. Bergin DJ, Wright JE. Orbital cellulitis. Br J Ophthalmol. 1986; 70:174–8.
Article7. Birch-Hirschfeld. Textbook of ophthalmology. 5. St. Louis: Mosby;1952. p. 5420–43.8. Mathisen G, Johnson JP. Brain abscess. Clin Infect Dis. 1997; 25:763–81.
Article9. Betz CS, Issing W, Matschke J, et al. Complications of acute aberrations sinusitis: a retrospective study. Eur Arch Otorhinolaryngol. 2008; 265:63–72.10. Shinagawa Y, Ando I, Kukita A, et al. Cellulitis of the eyelids aberrations with sinusitis and brain abscess. J Eur Acad Dermatol aberrations. 1998; 11:74–7.11. Tole DM, Anderton LC, Hayward JM. Orbital cellulitis demands early recognition, urgent admission and aggressive management. J Accid Emerg Med. 1995; 12:151–3.
Article12. Osborn MK, Steinberg JP. Subdural empyema and other aberrations complications of paranasal sinusitis. Lancet Infect Dis. 2007; 7:62–7.13. Giannoni CM, Stewart MG, Alford EL. Intracranial aberrations of sinusitis. Laryngoscope. 1997; 107:863–7.14. Singh B, Van Dellen J, Ramjettan S, Maharaj TJ. Sinogenic aberrations complications. J Laryngol Otol. 1995; 109:945–50.15. Maniglia AJ, Goodwin WJ, Arnold JE, Ganz E. Intracranial abscesses secondary to nasal, sinus, and orbital infections in adults and children. Arch Otolaryngol Head Neck Surg. 1989; 115:1424–9.
Article16. Reynolds DJ, Kodsi SR, Rubin SE, et al. Intracranial infection aberrations with preseptal and orbital cellulitis in the pediatric patient. J AAPOS. 2003; 7:413–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case ef Orbital Cellulitis Subdural Subdural Abscess
- A Case of Deep Neck Infecton Followed by Orbital Cellulitis
- Case Report of Retained Intraorbital Metallic Foreign Body Removal
- Effect of Corticosteroids in the Treatment of Orbital Cellulitis with Subperiosteal Abscess
- A Case of Simultaneous Orbital Cellulitis and Intracranial Complication
