A Case of Typical Cogan's Syndrome with Aortitis
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. yn35@snu.ac.kr
- 3Department of Internal Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Abstract
- Cogan's syndrome can accompany a variety of systemic vasculitides including aortitis. A 45-year-old woman with a history of typical Cogan's syndrome presented with orthopnea and exertional dyspnea. Echocardiography demonstrated severe aortic valve insufficiency. Computed tomographic angiography demonstrated active vasculitis affecting the ascending and descending aortas and also showed stenosis of the left subclavian artery, both renal arteries, the celiac axis, the superior mesenteric artery, and the right common iliac artery. She received high dose corticosteroid and then underwent an aortic valve replacement. This is the first case of Cogan's syndrome with aortitis in Korea.
Keyword
MeSH Terms
Figure
-
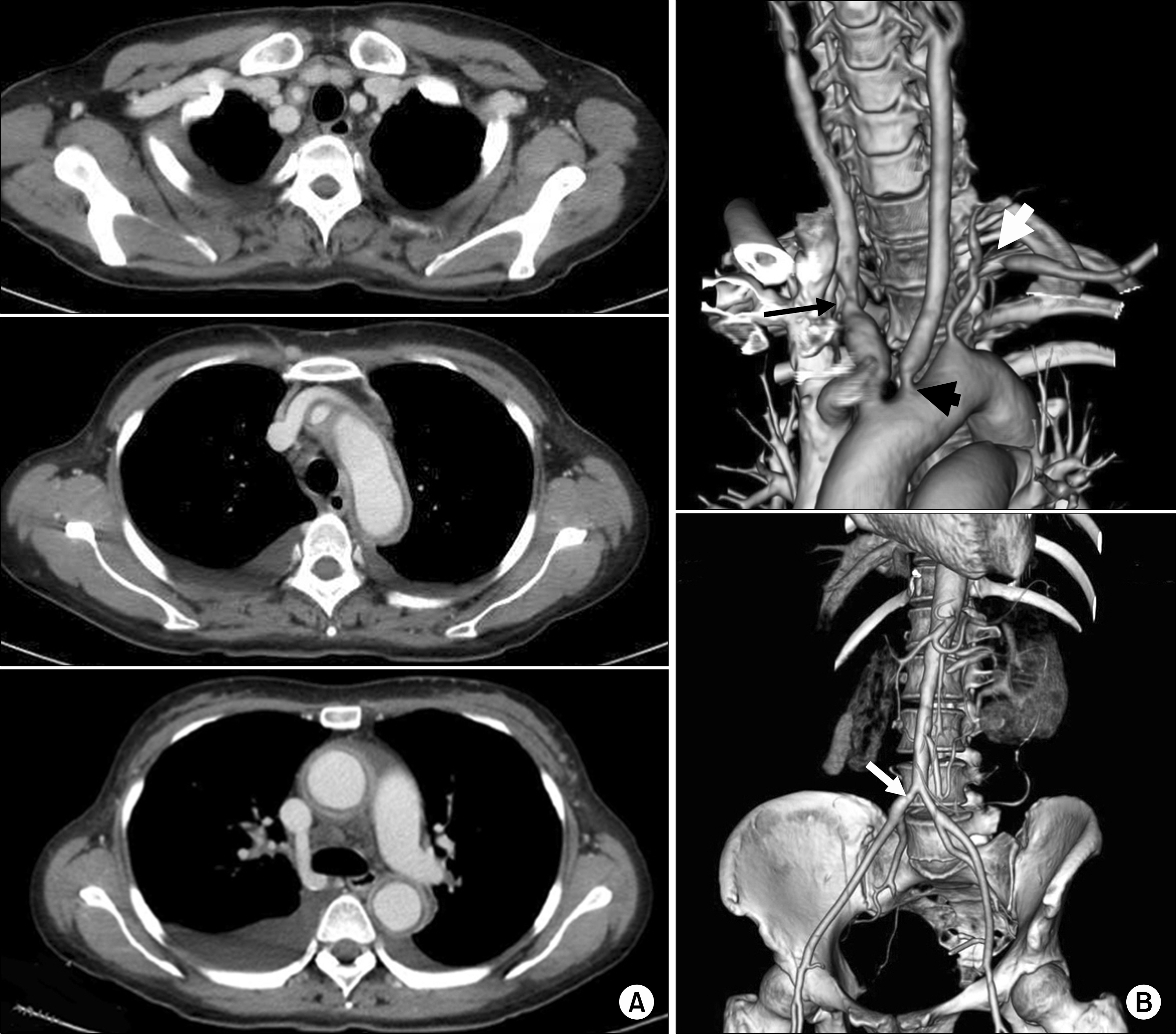
Fig. 1. Initial axial views of computed tomographic angiography revealed a thickened vascular wall with delayed enhancement in the right carotid artery, aortic arch, and descending aorta (A). The 3-D reconstruction images showed focal or diffuse stenotic lesions of the major branches of the aortic arch and abdominal aorta (B). Black thick arrow, the left common carotid artery; black thin arrow, the right innominate artery and common carotid artery; white thick arrow, the left subclavian artery; white thin arrow, the right common iliac artery.
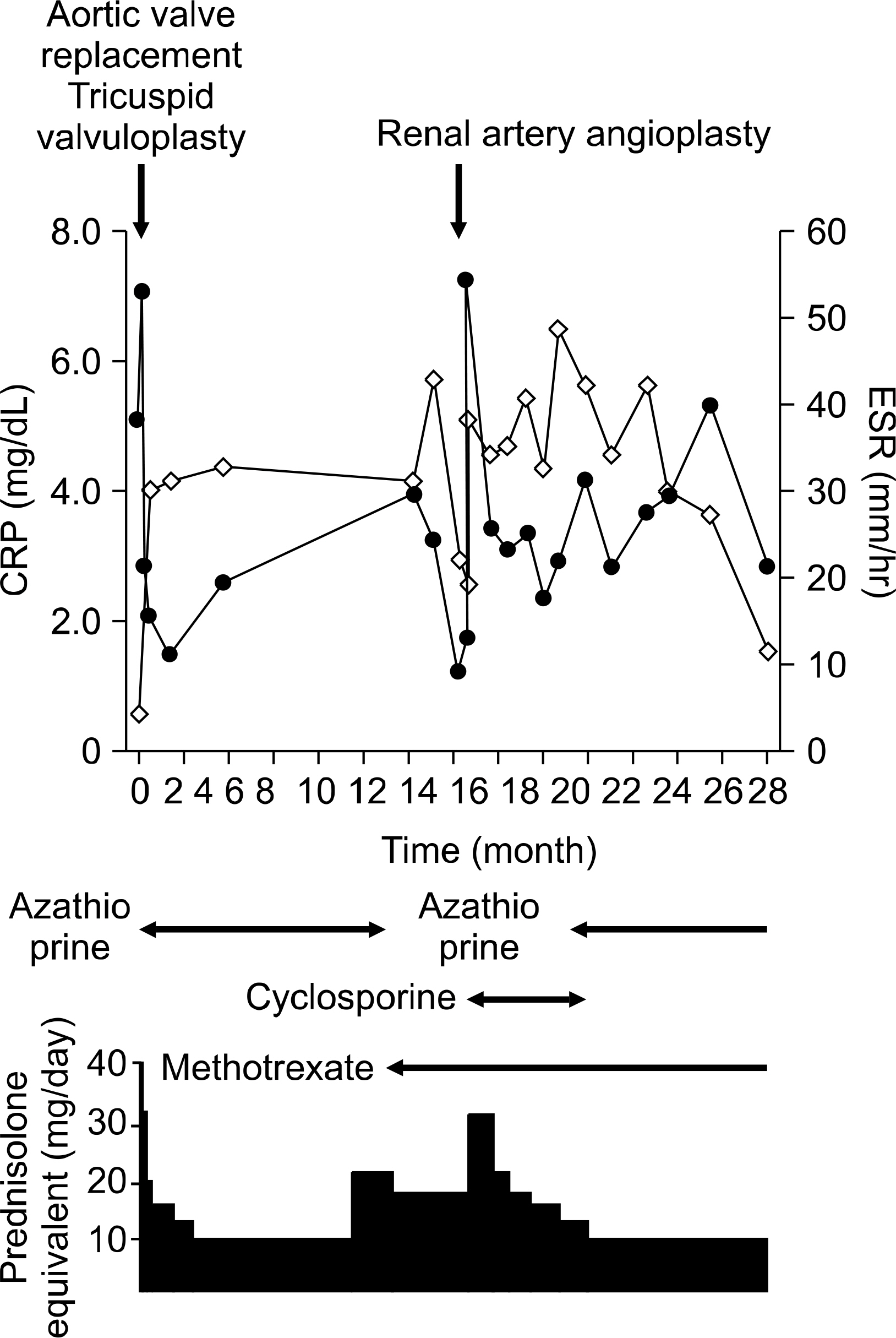
Fig. 2. The time-course of CRP and ESR levels during the immunosuppressive treatment of the patient. The dosage of azathioprine was increased to 150 mg/day, that of cyclosporine to 100 mg/day, and that of methotrexate to 17.5 mg/week. black circles (), CRP; white diamonds (), ESR.

Fig. 3. Computed tomographic angiography taken after 21 months still revealed active aortitis.
Reference
-
1). Grasland A., Pouchot J., Hachulla E., BleAtry O., Papo T., Vinceneux P. Study Group for Cogan's Syndrome. Typical and atypical Cogan's syndrome: 32 cases and review of the literature. Rheumatology (Oxford). 2004. 43:1007–15.
Article2). Gluth MB., Baratz KH., Matteson EL., Driscoll CL. Cogan syndrome: a retrospective review of 60 patients throughout a half century. Mayo Clin Proc. 2006. 81:483–8.
Article3). Mazlumzadeh M., Matteson EL. Cogan's syndrome: an audiovestibular, ocular, and systemic autoimmune disease. Rheum Dis Clin North Am. 2007. 33:855–74.
Article4). Chang WU., Shyn KH. Syndrome of nonsyphilitic interstitial keratitis and vestibuloauditory symptoms (cogan's syndrome). J Korean Opthalmol Soc. 1976. 17:337–40.5). Lee H., Yum DH., Shin MH., Chae SY., Suh BD. A case of Cogan's syndrome. Korean J Otolaryngol-Head Neck Surg. 1988. 31:113–7.6). Kim SJ., Han YG. A case of atypical Cogan syndrome with late-onset corneal involvement. J Korean Ophthalmol Soc. 2004. 45:310–4.7). Park JR., Rho YH., Choi SJ., Im GJ., Jung HH., Lee YH, et al. A case of Cogan's syndrome with antibodies to Ro (SS-A) and La (SS-B) antigen. J Korean Rheum Assoc. 2006. 13:82–5.8). Murphy G., Sullivan MO., Shanahan F., Harney S., Molloy M. Cogan's syndrome: present and future directions. Rheumatol Int. 2009. 29:1117–21.
Article9). Kondo Y., Ito S., Ohi Y., Satou H., Hiraoka T., Tsuboi H, et al. Atypical Cogan's syndrome with aortitis. Intern Med. 2009. 48:1093–7.
Article10). Jolly M., Curran JJ. Infliximab-responsive uveitis and vasculitis in a patient with Takayasu arteritis. J Clin Rheumatol. 2005. 11:213–5.
Article11). Maruyoshi H., Toyama K., Kojima S., Kawano H., Ogata N., Miyamoto S, et al. Sensorineural hearing loss combined with Takayasu's arteritis. Intern Med. 2005. 44:124–8.
Article12). Arend WP., Michel BA., Bloch DA., Hunder GG., Calabrese LH., Edworthy SM, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990. 33:1129–34.
Article13). Ghadban R., Couret M., Zenone T. Efficacy of infliximab in Cogan's syndrome. J Rheumatol. 2008. 35:2456–8.
Article14). Langford CA. Drug insight: anti-tumor necrosis factor therapies for the vasculitic diseases. Nat Clin Pract Rheumatol. 2008. 4:364–70.
Article
