A Case of Cogan's Syndrome With Angina
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Sahmyook Medical Center, Seoul Adventist Hospital, Seoul, Korea. mulgang@gmail.com
- KMID: 2225169
- DOI: http://doi.org/10.4070/kcj.2010.40.12.680
Abstract
- Cogan's syndrome is a rare systemic inflammatory disease and can be diagnosed on the basis of typical inner ear and ocular involvement with the presence of large vessel vasculitis. We report a case of Cogan's syndrome with stable angina resulting from coronary ostial stenosis caused by aortitis.
Keyword
MeSH Terms
Figure
-
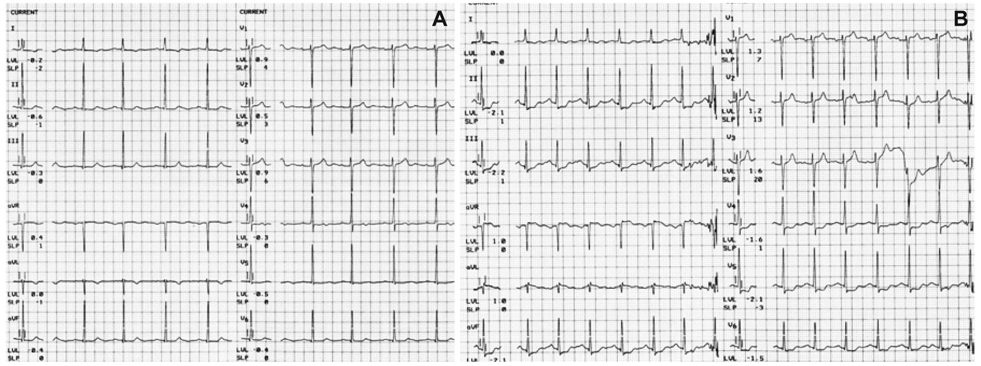
Fig. 1 Exercise electrocardiogram. A: baseline electrocardiogram shows normal sinus rhythm with nonspecific ST-T changes. B: electrocardiogram during exercise at Bruce protocol stage 2 reveals significant ST segment depressions at lead II, III, aVF, V4, V5, V6.
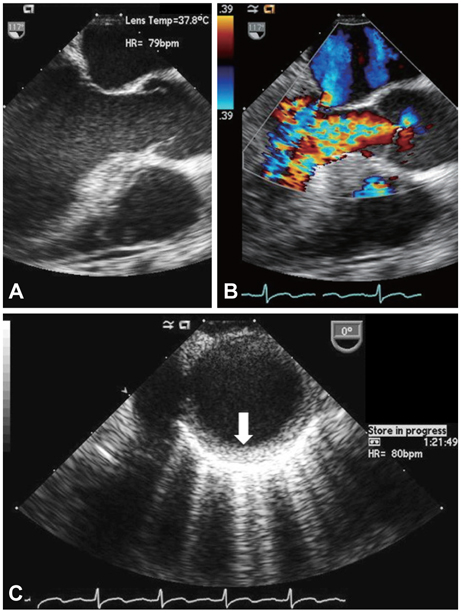
Fig. 2 Transesophageal echocardiogram shows retracted tips of aortic cusps in systolic phase (A), moderate aortic regurgitation in diastolic phase (B), and increased wall thickening at the descending thoracic aorta (C). Arrow indicates thickened intima.

Fig. 3 Angiography shows ostial left main stenosis (A), ostial right coronary stenosis (B), and bilateral subclavian stenosis (C). A: right anterior oblique view. B: left anterior oblique view. C: anteroposterior view.
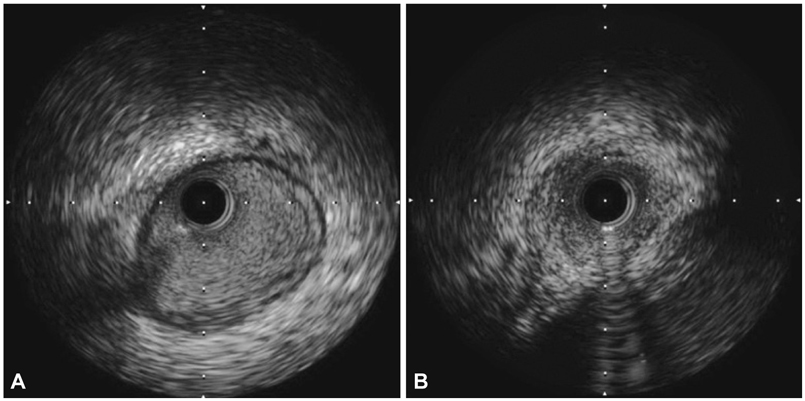
Fig. 4 Intravascular ultrasound shows increased intimal thickening at distal left main coronary (A) and negative remodeling with stenosis at ostial left main coronary artery (B).
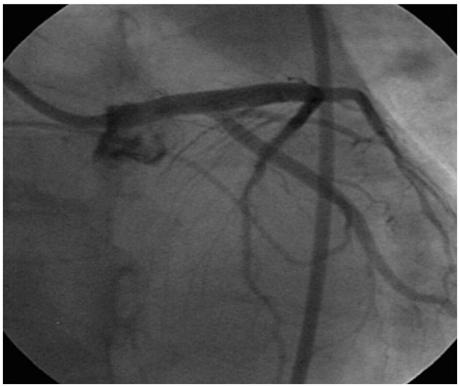
Fig. 5 Angiography after successful stenting shows widened left main ostium.
Reference
-
1. Mazlumzadeh M, Matteson EL. Cogan's syndrome: an audiovestibular, ocular, and systemic autoimmune disease. Rheum Dis Clin North Am. 2007. 33:855–874.2. Chynn EW, Jakobiec FA. Cogan's syndrome: ophthalmic, audiovestibular, and systemic manifestations and therapy. Int Ophthalmol Clin. 1996. 36:61–72.3. Grasland A, Pouchot J, Hachulla E, Bletry O, Papo T, Vinceneux P. Typical and atypical Cogan's syndrome: 32 cases and review of the literature. Rheumatology. 2004. 43:1007–1015.4. Haynes BF, Kaiser-Kupfer MI, Mason P, Fauci AS. Cogan syndrome: studies in thirteen patients, long-term follow-up, and a review of the literature. Medicine. 1980. 59:426–441.5. Vollertsen RS, McDonald TJ, Younge BR, Banks PM, Stanson AW, Illstup DM. Cogan's syndrome: 18 cases and a review of the literature. Mayo Clin Proc. 1986. 61:344–361.6. Gluth MB, Baratz KH, Matteson EL, Driscoll CL. Cogan syndrome: a retrospective review of 60 patients throughout a half century. Mayo Clin Proc. 2006. 81:483–488.7. Raza K, Karokis D, Kitas GD. Cogan's syndrome with Takayasu's arteritis. Br J Rheumatol. 1998. 37:369–372.8. Chun KJ, Kim SI, Na MA, Choi JH. Bilateral ostial coronary artery lesions in a patient with Takayasu's arteritis. Korean Circ J. 2004. 34:118–119.9. Park JS, Lee HC, Lee SK, et al. Takayasu's arteritis involving the ostia of three large coronary arteries. Korean Circ J. 2009. 39:551–555.10. Riente L, Taglione E, Berrettini S. Efficacy of methotrexate in Cogan's syndrome. J Rheumatol. 1996. 23:1830–1831.11. Orsoni JG, Zavota L, Vincenti V, Pellistri I, Rama P. Cogan syndrome in children: early diagnosis and treatment is critical to prognosis. Am J Ophthalmol. 2004. 137:757–758.12. McCallum RM. Cogan's syndrome. Current Ocular Therapy. 1993. 4th ed. Philadelphia: WB Saunders Company;410.
