J Korean Soc Spine Surg.
2001 Mar;8(1):46-52.
The Sagittal Balance and Compensatory Mechanisms in Lumbar Spinal Stenosis
- Affiliations
-
- 1Department of Orthopedic Surgery, Paik Hospital, Inje University, Pusan, Korea. osman64@unitel.co.kr
Abstract
-
PURPOSE: To evaluate the sagittal alignment and the main factors contributing to sagittal compensatory mechanism in lumbar stenosis.
MATERIALS AND METHODS
63 patients of spinal stenosis surgically treated were evaluated using 14x36 inch standing lateral films. The global sagittal balance was measured with C7 plumb line and hip flexion angle. The thoracic kyphosis, lumbar lordo-sis and pelvic tilting angle were compared to each of normal korean values to find out main factors participating in compensatory mechanism. At last follow-up, at least 6 months after surgery, the changes of sagittal parameters and global balance were evaluated according to the correction amount of pathologic segments angle to understand the compensatory mechanism and its contributing factors.
RESULTS
The C7 plumb line was +3.04 cm(/0.91 SD), thoracic kyphosis 30.0dgree(/12.1), lumbar lordosis 43.1dgree(/14.7) and pelvic tilting angle 21.7dgree(/8.2). All patients except 8 showed global compensation state. The differences compared to normal korean values were 10 dgree of pelvic tilting angle and 2dgreeof thoracic kyphosis. Pelvic tilting angle was more contributing factor of compensatory mechanism than thoracic kyphosis. At last follow up, 14 patients surgically corrected 5dgreeor more showed significant posterior shift of C7 plumb line and increased lumbar lordosis(p<0.05). 11 patients aggravated 5dgree or more showed significant increase of adjacent segment angle to participate in compensatory mechanism(p<0.05).
CONCLUSION
Most lumbar spinal stenosis patients showed compensated sagittal balance state. Adjacent segments and pelvic tilting were thought as main contributing factors of compensation mechanism.
MeSH Terms
Figure
-
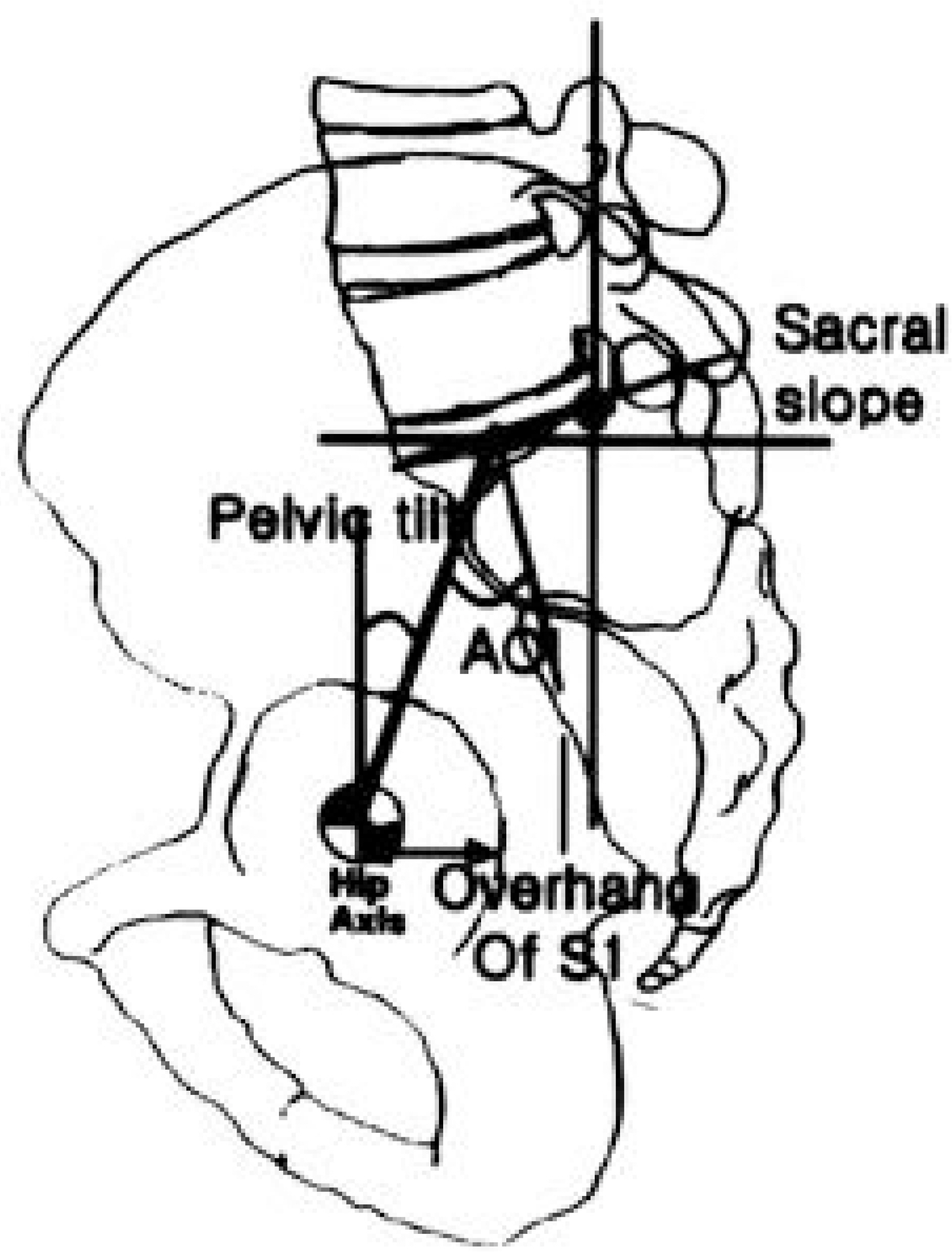
Fig. 1. Angle of incidence(AOI) is sum of pelvic tilting angle and sacral slope.
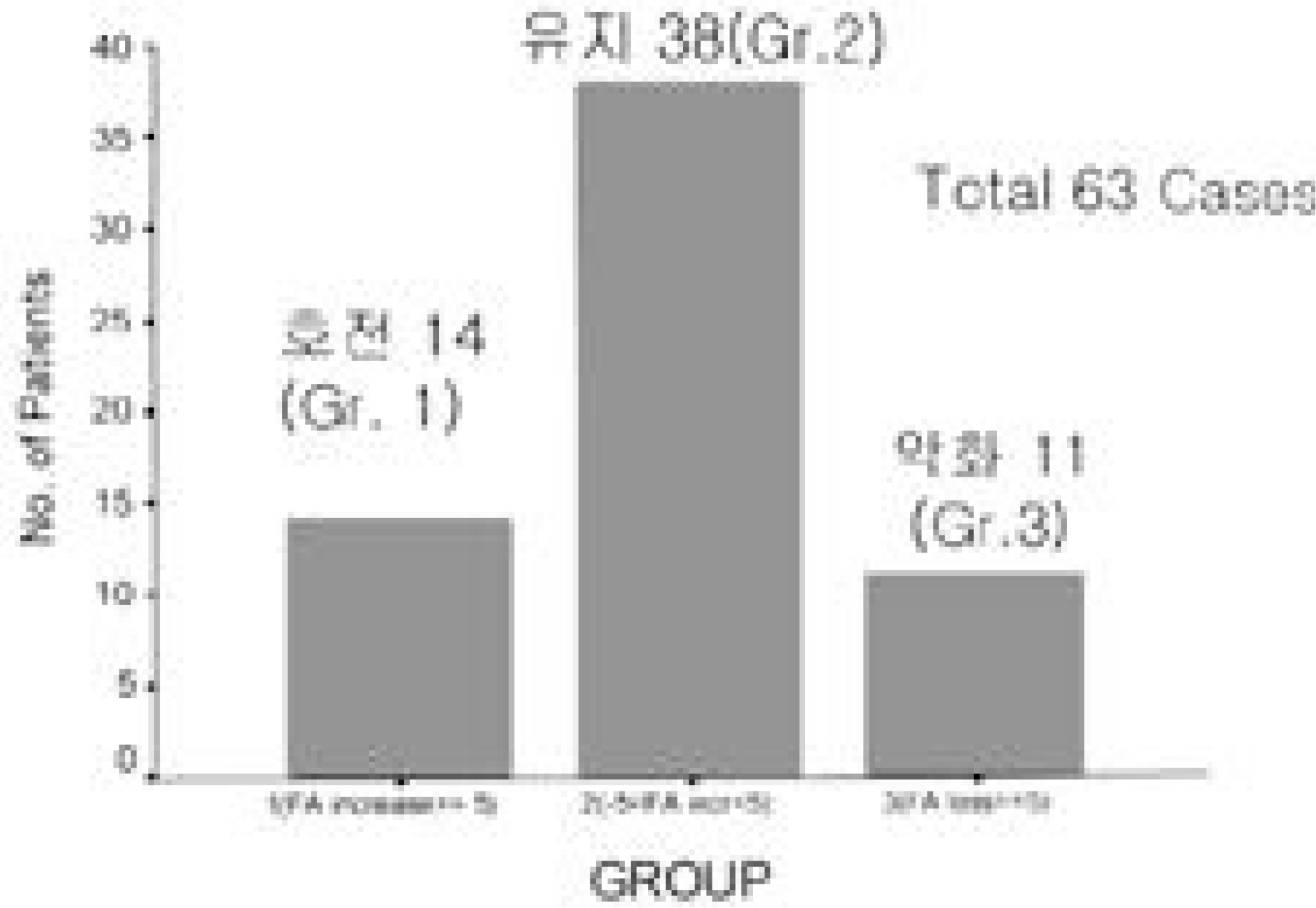
Fig. 2. Results of surgery. Among the total 63 cases, the fused segment’s lordosis angle(FA) was increased at least 5°(group 1) in 14 cases, decreased 5° or more(group 3) in 11 cases. In 38 cases, the changes were less than 5°(group 2).
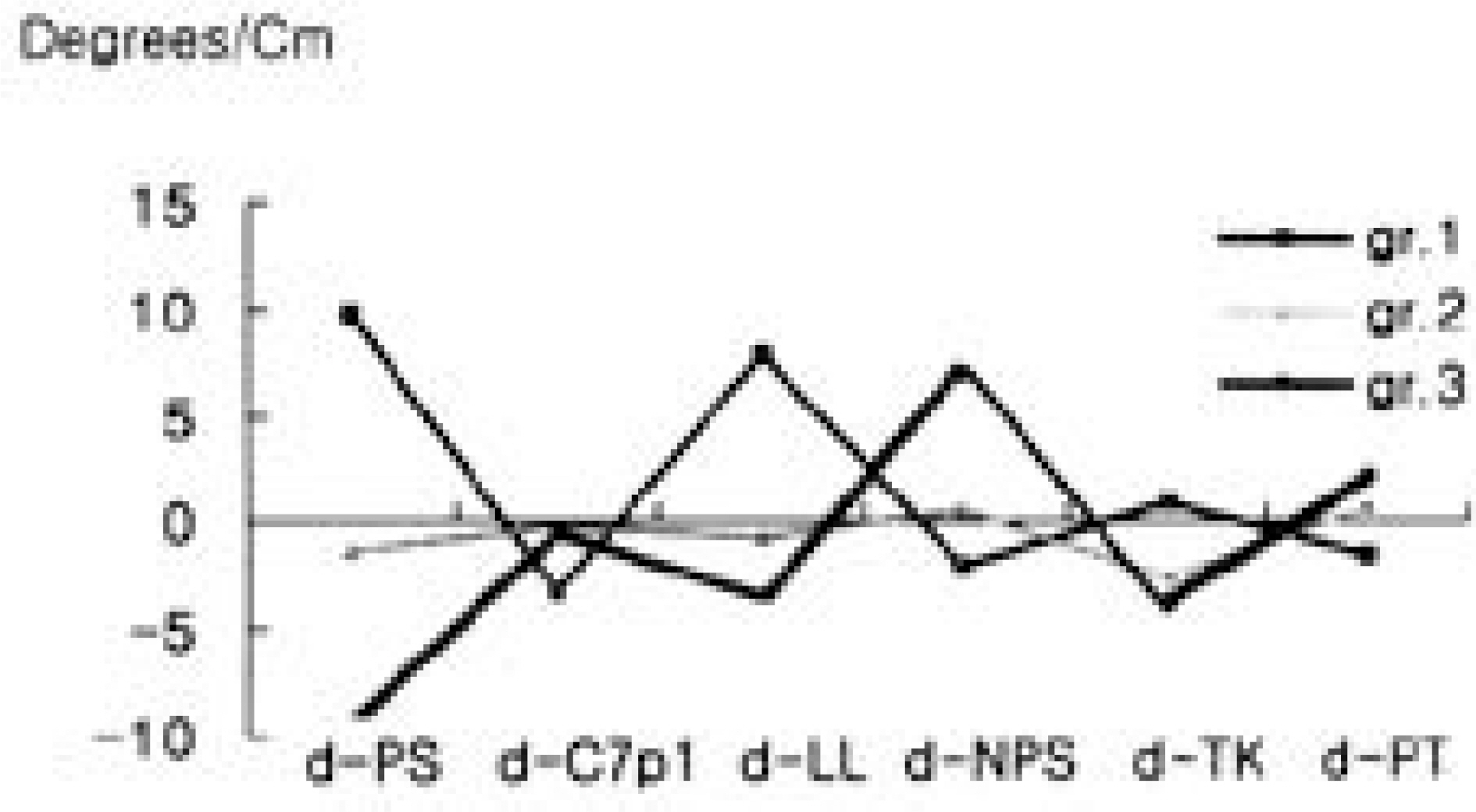
Fig. 3. The changes of sagittal parameters after surgery and follow-up. In group 1, the mean 9.9°increase of pathologic segments angle(d-PS) influenced to other parameters to be more comfortable. But in group 3, the other parameters were worsen especially the non-pathologic segments angle(d-NPS, adjacent segment’s angle) which was statistically significant.
Reference
-
1). 이종서, 오원환, 정성수, 이상국, 이종윤. 정상척추의 시상면 정렬의분석. 대한정형외과학회지. 34:949–954. 1999.2). Booth KC, Bridwell KH, Lenke LG, Baklus CR, Blanke KM. Complication and Predictive Factors for The Successful Treatment of Flatback Deformity(Fixed Sagittal Imbalance). Spine. 24(16):1712–1725. 1999.3). Chernukha KV, Dafner RH and Reigel DH. Lumbar lordosis measurement. Spine. 23(1):74–80. 1998.
Article4). Fernand R and Fox DE. Evaluation of lumbar lordosis. Spine. 10(9):799–803. 1985.
Article5). Hardacker JW, Shuford RF, Capicotto PN and Pryor PW. Radiologic standing cervical segmental alignment in adult volunteers without neck symtoms. Spine. 22(13):1472–1480. 1997.6). Holt RT, Dopf CA, Isaza JE, Rahn KA, Crawford MK and Kostuik JP. Adult Kyphosis: The Adult Spine. Principles and Practice. 2nd ed. Lippincott-Raven Inc;p. 1537–1878. 1997.7). Jackson RP. The Sagittal plane-from birth to grave: Spi-nopelvic alignment and balance. What process have we made in treating spinal deformity in the last ten years? SRS CME course. 1997.8). Jackson RP and McManus AC. Radologic Analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex and size. Spine. 19(4):1611–1618. 1994.9). Legaye J, Dubal-Beaupere G, Hecquet J and Marty C. Pelvic Incidence: A fundamental pelvic parameter for three dimensional regulation of spinal sagittal curves. European spine J. 7(2):99–103. 1998.10). Lenke LG, Linville DA and Bridwell KH. Sagittal Balance Consideration in Adult. Revision Spine Surgery. 1st ed. Mosby Inc;p. 752. 1999.11). Mark Bernhardt. Normal spinal anatomy: Normal sagittal plane alignment. The Textbook of Spinal Surgery. 2nd ed. Lippincott-Raven Inc;p. 185–191. 1997.12). Schlegel JD, Smith JA and Schleusener RL. Lumbar Motion Segement Pathology Adjacent to Thoracolumbar, Lumbar, and Lumbosacral Fusions. Spine. 21(8):970–981. 1996.13). Stokes IAF. Three-dimensional terminology of spinal deformity. Spine. 19(2):236–248. 1994.
Article
