J Korean Acad Periodontol.
2009 Dec;39(4):437-441.
CTG and restoration in treatment of gingival recession associated with a cervical lesion: report of three cases
- Affiliations
-
- 1Department of Periodontology, School of Dentistry, Kyungpook National University, Daegu, Korea. leejm@knu.ac.kr
Abstract
- PURPOSE
The purpose of this report is to show three cases treated by an intergrated periodontal and restorative dentistry approach. METHODS: Three patients with Miller Class I gingiva recessions associated with cervical lesions were enrolled for treatment. Two patients received a connective tissue graft and resin modified glass ionomer, and one patient was treated with a connective tissue graft, resin restoration. Keratinized gingiva and relative gingival recession were measured. RESULTS: The mean reduction of relative gingival recession was 3.7 mm, and the mean keratinized gingiva increase was 2.5 mm. The percentage of root coverage was 80% in average. No signs of gingival inflammation or bleeding on probing were seen. The patients were satisfied with the final esthetics and had no more dentin hypersensitivity. CONCLUSIONS: This report indicates that teeth with Miller Class I gingival recession associated with cervical lesions can be successfully treated by a connective tissue graft combined with restorative dentistry. However, longitudinal randomized controlled clinical trials must be performed to support this approach.
MeSH Terms
Figure
-

Figure 1 Preoperative view.
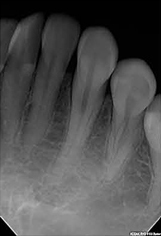
Figure 2 Radiographic finding.

Figure 3 Resin-ionomer restoration.
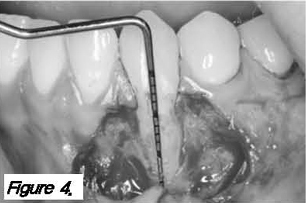
Figure 4 Recipient site preparation.

Figure 5 Connective tissue suture.

Figure 6 Postoperative view after 2 weeks.

Figure 7 Postoperative view after 6 month.

Figure 8 Preoperative view.

Figure 9 Recipient site preparation.

Figure 10 Resin-ionomer restoration.

Figure 11 Connective tissue graft.

Figure 12 Postoperative view after 2 weeks.

Figure 13 Postoperative view after 4 Month.

Figure 14 Preoperative view.

Figure 15 Connective tissue suture.

Figure 16 Postoperative view after 2 years.
Reference
-
1. Wennström JL. Mucogingival therapy. Ann Periodontol. 1996. 1:671–701.
Article2. Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: Prevalence, severity, and extent of gingival recessions. J Periodontol. 1992. 63:489–495.
Article3. Serino G, Wennström JL, Lindhe J, Enertoh L. The prevalence and distribution of gingival recession in subjects with high standard of oral hygiene. J Clin Periodontol. 1994. 21:57–63.
Article4. Sangnes G, Gjermo P. Prevalence of oral soft and hard tissue lesions related to mechanical toothcleansing procedures. Community Dent Oral Epidemiol. 1976. 4:77–83.
Article5. Toffenetti F, Vanini L, Tammaro S. Gingival recessions and noncarious cervical lesions: A soft and hard tissue challenge. J Esthet Dent. 1998. 10:208–220.
Article6. Zucchelli G, Testori T, De Sanctis M. Clinical and anatomical factors limiting treatment outcomes of gingival recession: A new method to predetermine the line root coverage. J Periodontol. 2006. 77:714–721.
Article7. Matis BA, Cochran MA. Technique on restoring cervical lesions. Oper Dent. 2002. 27:525–527.8. Chan DC, Adkins J. Technique on restoring subgingival cervical lesion. Oper Dent. 2003. 29:350–353.9. Terry DA, Mcguire MK, Mclaren E, Fulton R, Swift EJ Jr. Perioesthetic approach to the diagnosis and treatment of carious and noncarious cervical lesions: Part II. J Esthet Restor Dent. 2003. 15:284–296.
Article10. Raetzke PB. Covering localized areas of root exposure employing the "envelope" technique. J Periodontol. 1985. 56:397–402.
Article11. Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol. 1985. 56:715–720.
Article12. Nelson SW. The subepithelial connective tissue graft. A bilaminar reconstructive procedure for the coverage of denuded root surfaces. J Periodontol. 1987. 58:95–102.13. Dragoo MR. Resin-ionomer and hybrid-ionomer cements: Part II, human clinical and histologic wound healing responses in specific periodontal lesions. Int J Periodontic Restorative Dent. 1997. 17:75–87.14. Scherer W, Dragoo MR. New subgingival restorative procedures with Geristore resin ionomer. Pract Periodontics Aesthet Dent. 1995. 7:1–4.15. White C Jr. Repair of a root resorption lesion, A case report. J Periodontol. 1998. 69:596–600.
Article16. Anderegg CR. The treatment of class III maxillary furcations using a resin-ionomer: A case report. J Periodontol. 1998. 69:948–950.
Article17. Bruno JF, Bowers GM. Histology of a human biopsy section following the placement of a subepithelial connective tissue graft. Int J Periodontics Restorative Dent. 2000. 20:225–231.18. Sasanaluckit P, Albustany KR, Doherty PJ, Williams DF. Biocompatibility of glass ionomer cements. Biomaterials. 1993. 14:906–916.
Article19. el Mallakh BF, Sarkar NK. Fluride release from glass-ionomer cements in de-ionized water and artificial saliva. Dent Mater. 1990. 6:118–122.
Article20. Breault LG, Fowler EB, Primack PD. Endodontic perforation repair with resin-ionomer: A case report. J Contemp Dent Pract. 2000. 1:48–59.21. Alkan A, Keskiner I, Yuzbasioglu E. Connective tissue grafting on resin ionomer in localized gingival recession. J Periodontol. 2006. 77:1446–1451.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effective Management of Multiple Non-carious Cervical Lesions with Gingival Recession and Dentin Hypersensitivity: Two Cases Report of Combined Restorative and Periodontal Approach
- Relationship of occlusion and gingival recession
- Treatment efficacy of gingival recession defects associated with non-carious cervical lesions: a systematic review
- Treatment of Multiple Gingival Recessions Using Vestibular Incision Subperiosteal Tunnel Access with Platelet-rich Fibrin: Two Cases Reports
- A combined approach to non-carious cervical lesions associated with gingival recession
