World J Mens Health.
2013 Aug;31(2):170-175.
Testosterone Deficiency with Erectile Dysfunction in Mongolian Men
- Affiliations
-
- 1Department of Surgery, School of Medicine, Health Sciences University of Mongolia and ADAM Urology and Andrology Clinic, Ulaanbaatar, Mongolia.
- 2Monos Medical Institute, Ulaanbaatar, Mongolia.
- 3Department of Urology, National University Hospital of Mongolia, Ulaanbaatar, Mongolia.
- 4Department of Biochemistry and Laboratory Medicine, School of Biomedicine, Health Sciences University of Mongolia, Ulaanbaatar, Mongolia. munkhtsetseg@hsum-ac.mn
Abstract
- PURPOSE
To detect the testosterone deficiency syndrome in Mongolian men over 40 years old with erectile dysfunction (ED).
MATERIALS AND METHODS
Total of 309 males over 40 years of age who received medical care at the ADAM Urology and Andrology Clinic from 2010 to 2011 were included in this study. An approval from the Ethics Committee of the Ministry of Health of Mongolia was obtained, and each study participant signed a consent form at the beginning of the study. The participants were assigned to either an ED group or a control group, depending on the results of the international index of erectile function (IIEF)-5 questionnaire. The ED group was further divided into three groups (moderate, severe, and very severe) based on the level of ED. The total testosterone (TT) levels were determined in the blood serum using a competitive enzyme-linked immunesorbent assay (ELISA) analytical system UBI Magiwel(TM) Testosterone Quantitative test, and free testosterone (FT) calculated as described by the Vermeulen calculation. Test samples were collected between 8:00 and 11:00 am in the mornings and testosterone deficiency syndrome was diagnosed based on the International Society for the Study of the Aging Male guidelines, particularly, if TT was < or =3.46 ng/ml or free testosterone FT was < or =0.072 ng/ml.
RESULTS
ED of moderate, severe, and very severe levels was diagnosed in 199 (64.41%) out of 309 participants. There was an inverse relationship between the main IIEF-5 score and age (r=-0.380, p<0.01). The average TT was 5.75+/-2.316 ng/ml and FT was 0.091+/-0.0084 ng/ml. Compared to the ED group, the control group had a higher TT level: 5.6440+/-1.177 ng/ml and 5.812+/-2.316 ng/ml, respectively. In the control group, the FT level was 0.061+/-0.0084 ng/ml, whereas it was 0.041+/-0.0076 ng/ml in the ED group.
CONCLUSIONS
Our study showed that most of the aging males who came to the clinic had moderate to very severe ED (64.55%). The levels of TT (5.644+/-1.177 ng/ml) and FT (0.041+/-0.0036 ng/ml) were significantly lower in ED patients (p<0.05). The testosterone deficiency syndrome was detected in 24.27% of the ED group.
Keyword
MeSH Terms
Figure
-
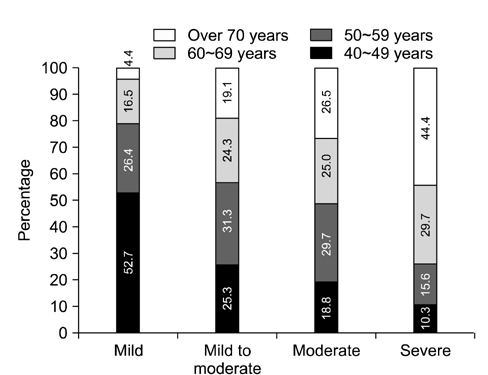
Fig. 1 Level of erectile dysfunction in different age groups.
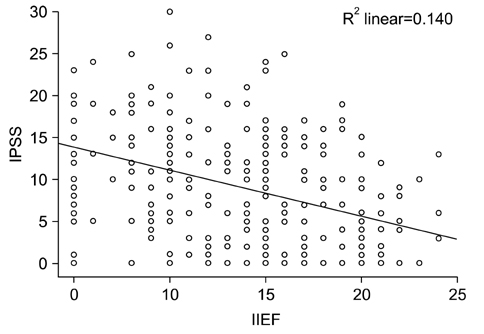
Fig. 2 Correlation of international index of erectile function (IIEF) and international prostate symptom score (IPSS) scores.
Reference
-
1. Gooren L, Lim PHC. Testosterone deficiency syndromepractical guidebook for general practitioners. Singapore: Creative plus;2010.2. Shabsigh R, Shah M, Sand M. Erectile dysfunction and men's health: developing a comorbidity risk calculator. J Sex Med. 2008; 5:1237–1243.
Article3. Haring R, Spielhagen C, Nauck M. Challenges in the measurement of serum testosterone concentrations as a biomarker of men's health. J Lab Med. 2011; 35:1–5.
Article4. Yassin AA, El-Sakka AI, Saad F, Gooren LJ. Lower urinary-tract symptoms and testosterone in elderly men. World J Urol. 2008; 26:359–364.
Article5. Haring R, Ittermann T, Völzke H, Krebs A, Zygmunt M, Felix SB, et al. Prevalence, incidence and risk factors of testosterone deficiency in a population-based cohort of men: results from the study of health in Pomerania. Aging Male. 2010; 13:247–257.
Article6. Torkler S, Wallaschofski H, Baumeister SE, Völzke H, Dörr M, Felix S, et al. Inverse association between total testosterone concentrations, incident hypertension and blood pressure. Aging Male. 2011; 14:176–182.
Article7. Mitchell Harman S. Testosterone, sexuality, and erectile function in aging men. J Androl. 2003; 24:6 Suppl. S42–S45.8. Haring R, Völzke H, Felix SB, Schipf S, Dörr M, Rosskopf D, et al. Prediction of metabolic syndrome by low serum testosterone levels in men: results from the study of health in Pomerania. Diabetes. 2009; 58:2027–2031.9. Hackett G, Cole N, Bhartia M, Kennedy D, Raju J, Wilkinson P. Testosterone replacement therapy with long-acting testosterone undecanoate improves sexual function and quality-of-life parameters vs. placebo in a population of men with type 2 diabetes. J Sex Med. 2013; 10:1612–1627.
Article10. Kang JI, Ham BK, Oh MM, Kim JJ, Moon DG. Correlation between serum total testosterone and the ams and iief questionnaires in patients with erectile dysfunction with testosterone deficiency syndrome. Korean J Urol. 2011; 52:416–420.
Article11. Rosen RC, Fisher WA, Eardley I, Niederberger C, Nadel A, Sand M. Men's Attitudes to Life Events and Sexuality (MALES) Study. The multinational Men's Attitudes to Life Events and Sexuality (MALES) study: I. Prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin. 2004; 20:607–617.12. Lau JT, Wang Q, Cheng Y, Yang X. Prevalence and risk factors of sexual dysfunction among younger married men in a rural area in China. Urology. 2005; 66:616–622.
Article13. Martin-Morales A, Sanchez-Cruz JJ, Saenz de, Rodriguez-Vela L, Jimenez-Cruz JF, Burgos-Rodriguez R. Prevalence and independent risk factors for erectile dysfunction in Spain: results of the Epidemiologia de la Disfuncion Erectil Masculina Study. J Urol. 2001; 166:569–574.
Article14. Meuleman EJ. Prevalence of erectile dysfunction: need for treatment? Int J Impot Res. 2002; 14:Suppl 1. S22–S28.
Article15. Jalil H, Mohammad M, Alireza G. Epidiomological study of prevalence and association of sexual dysfunction with potential risk factors. Int J of Urology. 2012; 19:Suppl 1. 271.16. Ahn TY, Park JK, Lee SW, Hong JH, Park NC, Kim JJ, et al. Prevalence and risk factors for erectile dysfunction in Korean men: results of an epidemiological study. J Sex Med. 2007; 4:1269–1276.
Article17. Corona G, Monami M, Rastrelli G, Aversa A, Tishova Y, Saad F, et al. Testosterone and metabolic syndrome: a meta-analysis study. J Sex Med. 2011; 8:272–283.
Article18. Lee YC, Liu CC, Huang CN, Li WM, Wu WJ, Yeh HC, et al. The potential impact of metabolic syndrome on erectile dysfunction in aging Taiwanese males. J Sex Med. 2010; 7:3127–3134.
Article19. Lee SH, Kim JC, Lee JY, Kim JH, Oh CY, Lee SW, et al. Effects of components of metabolic syndrome on sexual function in Korean BPH/LUTS patients. J Sex Med. 2009; 6:2292–2298.
Article20. Mondul AM, Rimm EB, Giovannucci E, Glasser DB, Platz EA. A prospective study of lower urinary tract symptoms and erectile dysfunction. J Urol. 2008; 179:2321–2326.
Article21. Mehraban D, Naderi GH, Yahyazadeh SR, Amirchaghmaghi M. Sexual dysfunction in aging men with lower urinary tract symptoms. Urol J. 2008; 5:260–264.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Obstructive Sleep Apnea and Testosterone Deficiency
- Correlation between Serum Total Testosterone and the AMS and IIEF Questionnaires in Patients with Erectile Dysfunction with Testosterone Deficiency Syndrome
- The Efficacy of a Combination of Phosphodiesterase Type 5 Inhibitor and Testosterone Replacement Therapy in Nonresponders to Phosphodiesterase Type 5 Inhibitor Mono-therapy
- The Relationship between Testosterone Deficiency and Men's Health
- Late Onset Hypogonadism and Lower Urinary Tract Symptoms: New Insights
