Embolic Infarction Associated with Cardiac Amyloidosis
- Affiliations
-
- 1Department of Neurology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. jongskim@amc.seoul.kr
- 2Department of Pathology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 2287718
- DOI: http://doi.org/10.3988/jcn.2005.1.1.92
Abstract
- Embolic cerebral infarction due to cardiac amyloidosis is rare. We report two patients with amyloidosis who developed cerebral infarcts. These embolic infarcts were probably related to cardiac involvement of amyloidosis, which was based on results of myocardial biopsy (Patient 1), and kidney biopsy and characteristic echocardiographic features including granular sparkling, restrictive cardiomyopathy and the presence of mural thrombus (Patient 2). Diffuse amyloid infiltration of the heart may have lead to impairment of myocardial function and subsequent mural thrombosis. Cardiomyopathy due to cardiac amyloidosis should be recognized as one of the causes of cardioembolic infarction.
Keyword
MeSH Terms
Figure
-
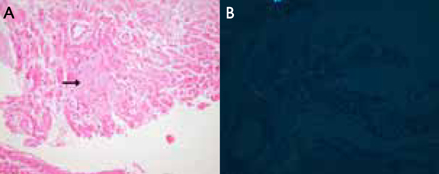
Figure 1 Endomyocardial biopsy findings of patient 1. (A) Deposition of amyloid is shown (arrow) (H&E ×200). (B) "Apple-green" birefringence under polarized light (Congo red stain ×400).
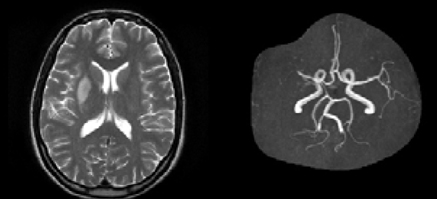
Figure 2 T2-weighted MRI of patient 1 shows cerebral infarcts in the right basal ganglia and corona radiata. MRA reveals near total occlusion or severe stenosis of the right distal M1 and proximal M2 portion of the MCA.
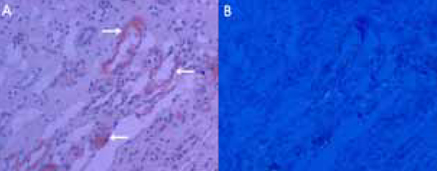
Figure 3 Kidney biopsy findings of patient 2. (A) Deposition of amyloid is shown in blood vessels of medulla (arrows) (H&E ×200). (B) "Apple-green" birefringence under polarized light (Congo red stain ×200).
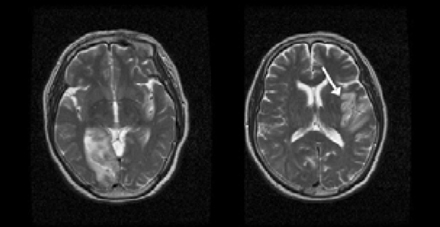
Figure 4 T2-weighted MRI of patient 2 shows cerebral infarcts in the right PCA and left MCA (arrow) territories.
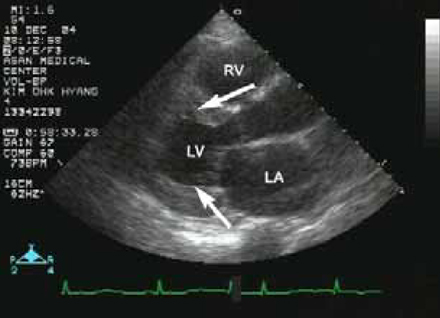
Figure 5 Echocardiographic findings of patient 2. Left ventricular wall is symmetrically thickened (arrows), and the size of the left ventricular cavity is small. Also observed are thickened interventricular septum, enlarged left atria and slightly increased myocardial echogenecity.
Reference
-
1. Sivaram CA, Jugdutt BI, Amy RWM, Basualdo CA, Haraphongse M, Shnitka TK. Cardiac amyloidosis: combined use of two-dimensional echocardiography and electrocardiography in noninvasive screening before biopsy. Clin Cardiol. 1985. 8:511–518.
Article2. International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders. Br J Haematol. 2003. 121:749–757.3. Falk RH, Comenzo RL, Skinner M. The systemic amyloidoses. N Engl J Med. 1997. 337:898–909.
Article4. Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser SL, Jameson JL. Harrison's principles of internal medicine. 2005. 16th ed. McGraw-Hill;2024–2030.5. Kushwaha SS, Fallon JT, Fuster V. Restrictive cardiomyopathy. N Engl J Med. 1997. 336:267–276.
Article6. Rice GP, Ebers GC, Newland F, Wysocki GP. Recurrent cerebral embolism in cardiac amyloidosis. Neurology. 1981. 31:904–907.
Article7. Owa M, Takei Y, Hashikura Y, Kawasaki S, Koyama M, Ikeda S. Recurrent cerebral embolism in a familial amyloid polyneuropathy patient who received partial liver transplantation from a living donor. Intern Med. 2001. 40:259–264.
Article8. Rahman JE, Helou EF, Gelzer-Bell R, Thompson RE, Kuo C, Rodriguez R, et al. Noninvasive diagnosis of biopsy-proven cardiac amyloidosis. J Am Coll Cardiol. 2004. 43:410–415.
Article9. Buja LM, Khoi NB, Roberts WC. Clinically significant cardiac amyloidosis. Clinicopathologic findings in 15 patients. Am J Cardiol. 1970. 26:394–405.10. Dardas PS, Tsikaderis DD, Mezilis N, Geleris P, Boudoulas H. Echocardiographic evidence of atrial myopathy in amyloidosis: a case report. Eur J Echocardiogr. 2002. 3:303–305.
Article11. Gertz MA, Lacy MQ, Dispenzieri A. Amyloidosis: recognition, confirmation, prognosis, and therapy. Mayo Clin Proc. 1999. 74:490–494.
Article12. Kothari SS, Ramakrishnan S, Bahl VK. Cardiac amyloidosis--an update. Indian Heart J. 2004. 56:197–203.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Contemporary Imaging Diagnosis of Cardiac Amyloidosis
- 5 cases of cardiac myxoma with neurologic manifestations
- Cardiac Amyloidosis Determines the Prognosis of Systemic Amyloidosis; Roles and Responsibilities of Cardiologist
- Treatment Response Evaluation of Cardiac Amyloidosis Using Serial T1- and T2-Mapping Cardiovascular Magnetic Resonance Imaging
- A Case of Systemic Amyloidosis
