J Clin Neurol.
2011 Sep;7(3):164-167. 10.3988/jcn.2011.7.3.164.
Spontaneous Carotid Cavernous Fistula in a Case with Protein S Deficiency that Newly Developed Ophthalmoplegia after Embolization
- Affiliations
-
- 1Department of Neurology, Seoul National University Hospital, Seoul, Korea. sb0516@snu.ac.kr
- KMID: 2287633
- DOI: http://doi.org/10.3988/jcn.2011.7.3.164
Abstract
- BACKGROUND
Carotid cavernous fistula (CCF) is an abnormal communication between the carotid artery and the cavernous sinus. The pathogenesis of spontaneous CCF remains unclear, although sinus thrombosis is known to be a predisposing factor for dural arteriovenous fistula. Because spontaneous CCFs are mainly of the dural type, we considered that thrombogenic conditions, such as, protein S deficiency might be associated with CCF.
CASE REPORT
A 42-year-old woman complained of conjunctival injection and retro-orbital pain that first appeared 1-month before visiting our hospital. She had no history of head trauma or intracranial surgery. Exophthalmos and chemosis were observed in her left eye, which also had lower visual acuity and higher intraocular pressure than the right eye. Magnetic resonance images and cerebral angiography revealed a left dural CCF. Her protein S was low, at 41% (normal range: 70-140%), but other hematologic values related to coagulation were normal. Her symptoms were relieved after initial transvenous coil embolization. However, a newly developed sixth-nerve palsy was detected 4 days after initial embolization. Follow-up angiography revealed a minimal shunt, and thus transvenous coil embolization was repeated. Two days later, the ophthalmoplegia started reducing, and 1-month later it had almost disappeared.
CONCLUSIONS
To the best of our knowledge, this is the first report of spontaneous dural CCF in a Korean patient with concurrent protein S deficiency. Interestingly, transient sixth-nerve palsy developed after transvenous coil embolization in this patient. This additional symptom caused by the residual fistula was relieved after additional transarterial embolization.
Keyword
MeSH Terms
-
Adult
Angiography
Carotid Arteries
Cavernous Sinus
Caves
Central Nervous System Vascular Malformations
Cerebral Angiography
Craniocerebral Trauma
Exophthalmos
Eye
Female
Fistula
Follow-Up Studies
Humans
Intraocular Pressure
Magnetic Resonance Spectroscopy
Ophthalmoplegia
Paralysis
Protein S
Protein S Deficiency
Sinus Thrombosis, Intracranial
Visual Acuity
Protein S
Figure
-
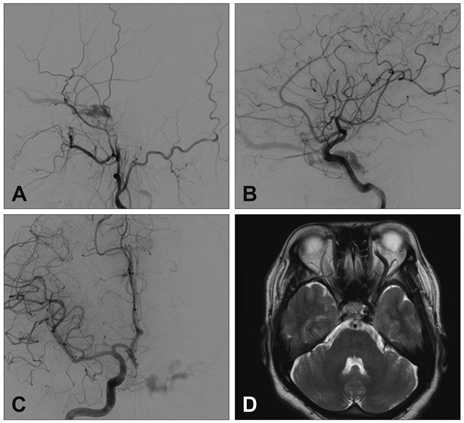
Fig. 1 Cerebral angiography images show a left CCF fed by the bilateral internal and external carotid arteries. A: Lateral arteriogram of left external carotid artery. B: Lateral arteriogram of left internal carotid artery. C: Anteroposterior arteriogram of right internal carotid artery. D: Magnetic resonance images indicate a prominent superior ophthalmic vein. CCF: carotid cavernous fistula.
Reference
-
1. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985. 62:248–256.
Article2. Uehara T, Tabuchi M, Kawaguchi T, Mori E. Spontaneous dural carotid cavernous sinus fistula presenting isolated ophthalmoplegia: evaluation with MR angiography. Neurology. 1998. 50:814–816.
Article3. Castoldi E, Hackeng TM. Regulation of coagulation by protein S. Curr Opin Hematol. 2008. 15:529–536.
Article4. Dykes AC, Walker ID, McMahon AD, Islam SI, Tait RC. A study of Protein S antigen levels in 3788 healthy volunteers: influence of age, sex and hormone use, and estimate for prevalence of deficiency state. Br J Haematol. 2001. 113:636–641.
Article5. Comp PC, Esmon CT. Recurrent venous thromboembolism in patients with a partial deficiency of protein S. N Engl J Med. 1984. 311:1525–1528.
Article6. Kim JS, Jeong SH, Kim DH, Kim J. Safety and feasibility of subcutaneous low molecular weight heparin for cerebral venous sinus thrombosis. J Clin Neurol. 2005. 1:134–141.
Article7. Aminoff MJ. Vascular anomalies in the intracranial dura mater. Brain. 1973. 96:601–612.
Article8. Suh DC, Lee JH, Kim SJ, Chung SJ, Choi CG, Kim HJ, et al. New concept in cavernous sinus dural arteriovenous fistula: correlation with presenting symptom and venous drainage patterns. Stroke. 2005. 36:1134–1139.
Article9. Handa J, Yoneda S, Handa H. Venous sinus occlusion with a dural arteriovenous malformation of the posterior fossa. Surg Neurol. 1975. 4:433–437.10. Haisa T, Yoshida S, Ohkubo T, Yoshikawa K, Machida T. Primary empty sella in association with superior sagittal sinus thrombosis and dural arteriovenous malformation. Case report. J Neurosurg. 1994. 81:122–125.
Article11. Yassari R, Jahromi B, Macdonald R. Dural arteriovenous fistula after craniotomy for pilocytic astrocytoma in a patient with protein S deficiency. Surg Neurol. 2002. 58:59–64. discussion 64.
Article12. Kojima T, Miyachi S, Sahara Y, Nakai K, Okamoto T, Hattori K, et al. The relationship between venous hypertension and expression of vascular endothelial growth factor: hemodynamic and immunohistochemical examinations in a rat venous hypertension model. Surg Neurol. 2007. 68:277–284. discussion 284.
Article13. Gerlach R, Yahya H, Rohde S, Böhm M, Berkefeld J, Scharrer I, et al. Increased incidence of thrombophilic abnormalities in patients with cranial dural arteriovenous fistulae. Neurol Res. 2003. 25:745–748.
Article14. Gerlach R, Boehm-Weigert M, Berkefeld J, Duis J, Raabe A, Seifert V, et al. Thrombophilic risk factors in patients with cranial and spinal dural arteriovenous fistulae. Neurosurgery. 2008. 63:693–698. discussion 698-699.
Article15. Izumi T, Miyachi S, Hattori K, Iizuka H, Nakane Y, Yoshida J. Thrombophilic abnormalities among patients with cranial dural arteriovenous fistulas. Neurosurgery. 2007. 61:262–268. discussion 268-269.
Article16. Preter M, Tzourio C, Ameri A, Bousser MG. Long-term prognosis in cerebral venous thrombosis. Follow-up of 77 patients. Stroke. 1996. 27:243–246.17. Kim DJ, Kim DI, Suh SH, Kim J, Lee SK, Kim EY, et al. Results of transvenous embolization of cavernous dural arteriovenous fistula: a single-center experience with emphasis on complications and management. AJNR Am J Neuroradiol. 2006. 27:2078–2082.18. Klisch J, Schipper J, Husstedt H, Laszig R, Schumacher M. Transsphenoidal computer-navigation-assisted deflation of a balloon after endovascular occlusion of a direct carotid cavernous sinus fistula. AJNR Am J Neuroradiol. 2001. 22:537–540.19. Klisch J, Huppertz HJ, Spetzger U, Hetzel A, Seeger W, Schumacher M. Transvenous treatment of carotid cavernous and dural arteriovenous fistulae: results for 31 patients and review of the literature. Neurosurgery. 2003. 53:836–856. discussion 856-857.
Article20. Nishino K, Ito Y, Hasegawa H, Kikuchi B, Shimbo J, Kitazawa K, et al. Cranial nerve palsy following transvenous embolization for a cavernous sinus dural arteriovenous fistula: association with the volume and location of detachable coils. J Neurosurg. 2008. 109:208–214.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Carotid-Cavernous Fistula in the Type IV Ehlers-Danlos Syndrome
- A Case of Spontaneous of Traumatic Carotid Cavernous Fistula After Carotid Angiography
- A Case of Carotid Cavernous Fistula Treated by Muscle and Polyurethane Foam Embolization: Case Report
- Central Retinal Vein Occlusion During Embolization for Carotid Cavernous Sinus Fistula
- Intraoperative Embolization of Dural Carotid-Cavernous Fistula: Case Report
