The Efficacy of Stereotactic Vacuum-assisted Biopsy and Needle Localization Vacuum-assisted Biopsy for Diagnosing Breast Microcalcification
- Affiliations
-
- 1Dr.Oh's Breast Center, Seoul, Korea. ohsemin2000@yahoo.co.kr
- KMID: 2286560
- DOI: http://doi.org/10.4048/jbc.2010.13.1.53
Abstract
- PURPOSE
This study was conducted to evaluate the efficacy of 2 percutaneous breast biopsy techniques for diagnosing microcalcification: stereotactic Vacuum-assisted biopsy (VAB) and needle localization VAB.
METHODS
Between November 2002 and September 2007, 138 patients underwent percutaneous breast biopsy for microcalcification. Of these, 59 patients underwent needle localization VAB and 79 patients underwent stereotactic VAB with using a prone-table mammographic unit, respectively. Patients with focally clustered microcalcification underwent stereotactic VAB. Patients with diffuse or deep seated microcalcification and patients with small breast underwent needle localization VAB. We retrospectively reviewed the characteristics of the lesions and the percutaneous biopsy results for all the cases.
RESULTS
Percutaneous biopsy was successful in 135 cases (97.8%). Of the 135 successfully performed cases, 34 cases (25.2%) were malignant and there were 4 (11.8%) underestimations. For the stereotactic VAB group, 13 of the successfully performed 76 cases (17.1%) were malignant and there were 2 (15.4%) underestimations. In needle localization VAB group, 21 (36.6%) of the 59 cases were malignant and there were 2 (9.5%) underestimations. There was no major complication in all the cases.
CONCLUSION
With using stereotactic VAB and needle localization VAB, we can biopsy accurately and safely in almost all cases with leaving only minimal scar. So, percutaneous biopsy can be considered as a substitute for surgical biopsy for microcalcification of the breast.
Keyword
Figure
-

Figure 1 Stereotactic vacuum-assisted biopsy with prone-type mammographic unit. The 11G mammotome needle is placed in the breast to acquire the specimen.

Figure 2 (A) Prefire stereo scout view: positioning the probe proximal to the lesion. (B) Postexamination view and specimen mammography. The microcalcification particles seen in the stereo-scout view (A) are not visible anymore in the postexamination view (Left). The specimen mammogram demonstrates calcifications in multiple cores (Right).
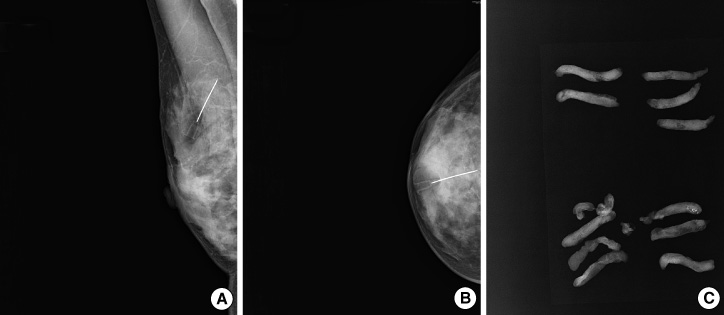
Figure 3 Needle localization vacuum-assisted biopsy. (A, B) After the needle was inserted into the lesion, the proper location must be warranted with mammography (lateral and cephalocaudal view). (C) Specimen mammography shows proper A B C acquisition of calcification.

Figure 4 Needle localization vacuum-assisted biopsy. The skin above the lesion must be marked before the acquisition of tissue.
Reference
-
1. Korean Central Cancer Registry. 2002 Annual report of the Korean Central Cancer Registry. 2003. Gwacheon: Ministry of Health and Welfare.2. Lee NS, Park WC, Lee DH, Song BJ, Kim JS, Oh SJ, et al. Diagnosis of non-palpable breast lesions with microcalcification by upright add-on type stereotactic vacuum-assisted biopsy. J Korean Breast Cancer Soc. 2004. 7:256–262.
Article3. Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL. Efficacy of screening mammography. A meta-analysis. JAMA. 1995. 273:149–154.
Article4. Jeong WB, Bum WK. Retrospective analysis of the needle localization biopsies for nonpalpable mammographic microcalcifications of the breast. J Korean Surg Soc. 1994. 46:335–341.5. Reynolds HE, Poon CM, Goulet RJ, Lazaridis CL. Biopsy of breast microcalcifications using an 11-guage directed vacuum-assisted devices. AJR Am J Radiol. 1998. 171:611–613.
Article6. Greenberg D, Johnston J, Hart R, Weston M, Benson-Cooper D. Stereotactic breast biopsy: an audit of 18 months at BreastScreen Auckland. Australas Radiol. 2003. 47:261–267.
Article7. Meloni GB, Becchere MP, Soro D, Feo CF, Profili S, Dettori G, et al. Percutaneous vacuum-assisted core breast biopsy with upright stereotactic equipment; indications, limitations and results. Acta Radiol. 2002. 43:575–578.
Article8. Burak WE, Owens KE, Tighe MB, Kemp L, Dinges SA, Hitchcock CL, et al. Vacuum-assisted stereotactic breast biopsy: histologic underestimation of malignant lesions. Arch Surg. 2000. 135:700–703.9. Burbank F. Stereotactic breast biopsy: comparison of 14- and 11-guage Mammotome probe performance and complication rates. Am Surg. 1997. 63:988–995.10. Kettritz U, Rotter K, Schreer I, Murauer M, Schulz-Wendtland R, Peter D, et al. Stereotactic vacuum-assisted biopsy in 2874 patients: a multicenter study. Cancer. 2004. 100:245–251.
Article11. Philpotts LE, Lee CH, Horvath LJ, Tocino I. Canceled stereotactic core-needle biopsy of the breast: analysis of 89 cases. Radiology. 1997. 205:423–428.
Article12. Parker SH, Burbank F, Jackman RJ, Aucreman CJ, Cardenosa G, Cink TM, et al. Percutaneous large-core breast biopsy: a multi-institutional study. Radiology. 1994. 193:359–364.
Article13. Brenner RJ, Bassett LW, Fajardo LL, Dershaw DD, Evans WP 3rd, Hunt R, et al. Stereotactic core-needle breast biopsy: a multi-institutional prospective trial. Radiology. 2001. 218:866–872.
Article14. Jackman RJ, Burbank F, Parker SH, Evans WP 3rd, Lechner MC, Richardson TR, et al. Stereotactic breast biopsy of nonpalpable lesions: determinants of ductal carcinoma in situ underestimation rates. Radiology. 2001. 218:497–500.
Article15. Jackman RJ, Rodriguez-Soto J. Breast microcalcifications: retrieval failure at prone stereotactic core and vacuum breast biopsy-frequency, causes, and outcome. Radiology. 2006. 239:61–70.
Article16. Liberman L, Smolkin JH, Dershaw DD, Morris EA, Abramson AF, Rosen PP. Calcification retrieval at stereotactic, 11-guage, directional, vacuum-assisted breast biopsy. Radiology. 1998. 208:251–260.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of Non-palpable Breast Lesions with Microcalcification by Upright Add-on Type Stereotactic Vacuum-assisted Biopsy
- Comparison of needle aspiration and vacuum-assisted biopsy in the ultrasound-guided drainage of lactational breast abscesses
- US-guided Vacuum-assisted Breast Biopsy with Air Localization for Patients with Microcalcifications
- Usefulness of Ultrasound-guided Mammotome Biopsy for Microcalcification
- US-Guided Vacuum-Assisted Biopsy of Microcalcifications in Breast Lesions and Long-Term Follow-Up Results
