Contralateral Breast Management Related to Breast Reconstruction in Korean Females
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Kyungpook National University, Graduate School of Medicine, Daegu, Korea. lambyang@paran.com
- 2Department of Surgery, Kyungpook National University, Graduate School of Medicine, Daegu, Korea.
- KMID: 2286539
- DOI: http://doi.org/10.4048/jbc.2010.13.2.147
Abstract
- PURPOSE
The final purpose of post mastectomy reconstruction is a balanced, symmetrical, pleasing appearance for both breasts. However, in cases where women have an unattractive breast, which may be small, ptotic or huge, remodeling of the contralateral breast may be desirable. Surgical options available for the contralateral breast included breast augmentation using implants, mastopexy, and reduction mammoplasty.
METHODS
All patients who underwent unilateral breast reconstruction at Kyungpook National University Hospital from September of 2006 to February of 2008 were included in this study. The methods of reconstruction included transverse rectus abdominis musculocutaneous flap, latissimus dorsi flap, and the use of implants. Contralateral procedures to achieve symmetry included augmentation, mastopexy, and reduction.
RESULTS
A total of 57 patients were evaluated, including 45 immediate, and 12 delayed reconstructions. Twenty-six of these patients underwent contralateral breast management (augmentation [12], mastopexy [11], and reduction [3]). The average age was 44.9 years and the mean follow up interval was 13 months. Most of the patients were satisfied with the symmetry, clothed appearance, nude appearance, aesthetics, and consistency. Sixty-six percent (8 of 12) of delayed reconstruction patients had a symmetry procedure performed on the opposite breast, compared with 40 percent (18 of 45) of the immediate-reconstruction patients. No complications were observed on the contralateral breasts undergoing symmetrization.
CONCLUSION
Contralateral management in breast reconstruction can provide symmetry with the reconstructed breast contour and aesthetically satisfactory results in a safe manner. Immediate symmetrization procedure also can avoid secondary operations and offer psychological benefits without delaying adjuvant therapy.
MeSH Terms
Figure
-
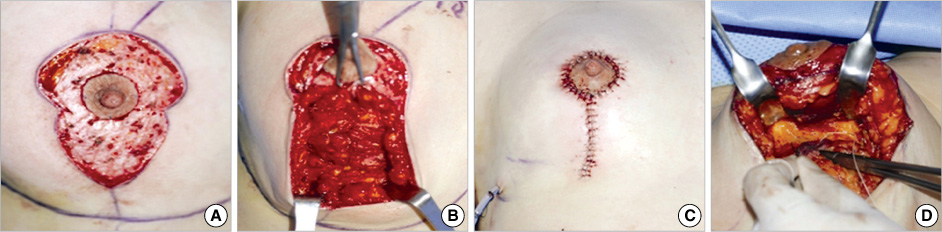
Figure 1 A vertical mastopexy for ptotic breast. (A) After deepithelization. (B) Pillars pulled together with inverted sutures. (C) Immediate postoperative view. (D) When both correction of ptosis and projection were needed, the inferior thoracic-based flap of the breast was transposed underneath and fixed to the pectoralis fascia for added projection.
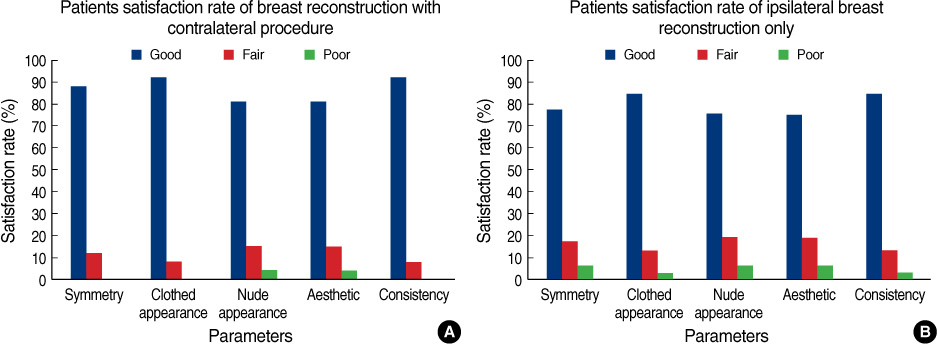
Figure 2 Satisfaction rate. The subjective analysis of results by patients indicated satisfaction with the combined procedure. Contralateral procedure group (A). Ipsilateral breast reconstruction only group (B).

Figure 3 (A, B) A 36-year-old woman with cancer of the left breast. (C, D) The same patient after skin sparing mastectomy. Immediate TRAM flap reconstruction and augmentation on contralateral breast were performed. Results 12 months postoperatively.
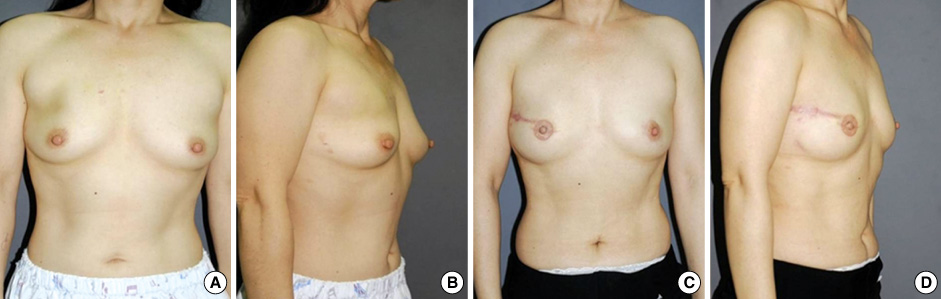
Figure 4 (A, B) A 36-year-old woman with cancer of the right breast. (C, D) The same patient after skin sparing mastectomy. Immediate breast reconstruction with a silicone implant and periareolar mastopexy on the contralateral breast were performed. Results 14 months postoperatively.
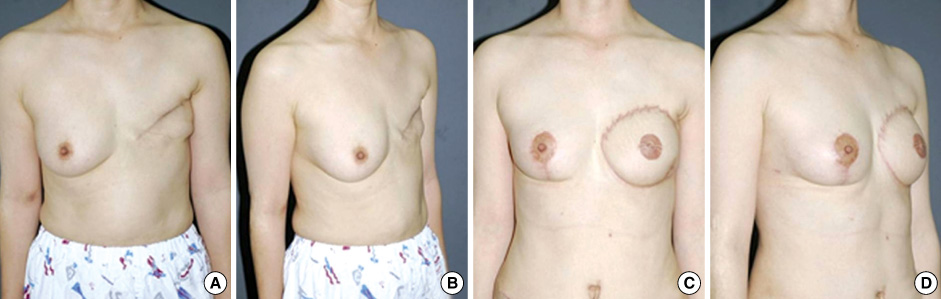
Figure 5 (A, B) A 47-year-old woman with cancer of the left breast. (C, D) The same patient after delayed TRAM flap reconstruction and vertical reduction on the contralateral breast. Results 13 months postoperatively.
Reference
-
1. Hartrampf CR, Scheflan M, Black PW. Breast reconstruction with a transverse abdominal island flap. Plast Reconstr Surg. 1982. 69:216–225.
Article2. Dinner MI, Dowden RV. Gant TD, Vasconez LO, editors. Management of the contralateral breast. Postmastectomy Reconstruction. 1988. 2nd ed. Baltimore: Williams & Wilkins;205–217.3. Losken A, Carlson GW, Bostwick J 3rd, Jones GE, Culbertson JH, Schoemann M. Trends in unilateral breast reconstruction and management of the contralateral breast: The Emory experience. Plast Reconstr Surg. 2002. 110:89–97.
Article4. Nahabedian MY. Managing the opposite breast: contralateral symmetry procedures. Cancer J. 2008. 14:258–263.
Article5. Ulusal BG, Cheng MH, Wei FC. Simultaneous endoscopic-assisted contralateral breast augmentation with implants in patients undergoing postmastectomy breast reconstruction with abdominal flaps. Plast Reconstr Surg. 2006. 118:1293–1302.
Article6. Petit JY, Rietjens M, Contesso G, Bertin F, Gilles R. Contralateral mastoplasty for breast reconstruction: a good opportunity for glandular exploration and occult carcinomas diagnosis. Ann Surg Oncol. 1997. 4:511–515.
Article7. Miller MJ, Rock CS, Robb GL. Aesthetic breast reconstruction using a combination of free transverse rectus abdominis musculocutaneous flaps and breast implants. Ann Plast Surg. 1996. 37:258–264.
Article8. Serletti JM, Moran SL. The combined use of the TRAM and expanders/implants in breast reconstruction. Ann Plast Surg. 1998. 40:510–514.
Article9. Stevenson TR, Goldstein JA. TRAM flap breast reconstruction and contralateral reduction of mastopexy. Plast Reconstr Surg. 1993. 92:228–233.
Article10. Lejour M, Jabri M, Deraemaecker R. Analysis of long-term results of 326 breast reconstructions. Clin Plast Surg. 1988. 15:689–701.
Article11. Restifo RJ. TRAM revisions and contralateral mammaplasties: the role of "mirror image" skin patterns. Semin Plast Surg. 2004. 18:245–253.
Article12. Chen JS. Simultaneous TRAM flaps with contralateral augmentation mammaplasty in breast reconstruction. ANZ J Surg. 2003. 73:A238.13. VanderKam VM, Achauer BM. Breast reconstruction: the contralateral breast. Plast Surg Nurs. 1996. 16:197–198. 19614. Murillo WL. Contralateral breast management in breast reconstruction. Semin Plast Surg. 2002. 16:77–91.
Article15. Graf R, Reis de Araujo LR, Rippel R, Neto LG, Pace DT, Biggs T. Reduction mammaplasty and mastopexy using the vertical scar and thoracic wall flap technique. Aesthetic Plast Surg. 2003. 27:6–12.
Article16. Ueda S, Tamaki Y, Yano K, Okishiro N, Yanagisawa T, Imasato M, et al. Cosmetic outcome and patient satisfaction after skin-sparing mastectomy for breast cancer with immediate reconstruction of the breast. Surgery. 2008. 143:414–425.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous TRAM Flap Breast Reconstruction with Contralateral Reduction Mammoplasty
- Breast Reconstruction Make Use of Contralateral Breast Tissue after Mastectomy
- Ultrasonographic Findings of Postoperative Change after Breast Reconstruction
- Selection of Implants in Unilateral Prosthetic Breast Reconstruction and Contralateral Augmentation
- Transabdominal Augmentation of Contralateral Breast in TRAM Breast Reconstruction
