Occult Breast Cancers Manifesting as Axillary Lymph Node Metastasis in Men: A Two-Case Report
- Affiliations
-
- 1Department of Surgery, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea.
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. 20110364@kuh.ac.kr
- KMID: 2286464
- DOI: http://doi.org/10.4048/jbc.2012.15.3.359
Abstract
- Occult breast cancer is a type of breast cancer without any symptoms on the breasts or any abnormalities upon radiologic examination such as mammography. In males, there are few cases of breast cancer, the rate of diagnosis of occult breast cancer is very low, and little is known about this disease. We experienced two cases of occult breast cancers manifesting as axillary lymph node metastasis in men. They had a palpable lesion on axillary area several years ago and had not seen a doctor about it. As such there was no abnormality on evaluations for cancer except for axillary lymph node showing signs of carcinoma (primary or metastatic) on biopsy and estrogen receptor-positive and progesterone receptor-positive on immunohistochemistry. The patients were diagnosed with occult breast cancer, and treatments were performed. Herein, we report the rare cases of occult breast cancers in men.
MeSH Terms
Figure
-

Figure 1 Mammography (A), breast ultrasound (B), and magnetic resonance imaging scans (C) do not show abnormalities in the breast. Positron emission tomography (D) shows malignant lymphadenopathy in right axilla without other suspicious malignant lesion.
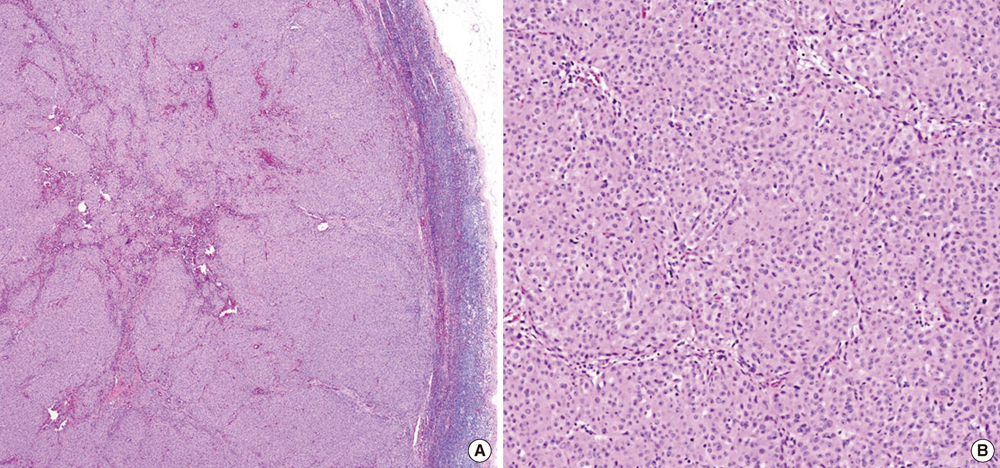
Figure 2 Case 1. Histopathologic examination of the lymph node specimen. It identify these as metastatic carcinoma in H&E stain (A, ×50; B, ×100).
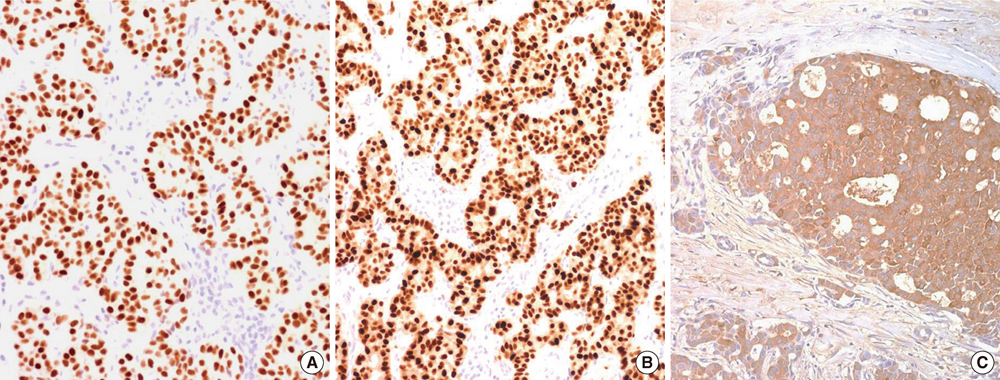
Figure 3 Case 2. Histopathologic examination of the lymph node specimen (immunohistochemical staining, ×200). It shows positive expression of estrogen receptor (A), progesterone receptor (B), and BRST-2 (C) in immunohistochemistry stain.
Cited by 1 articles
-
A Case Report of Male Occult Breast Cancer Manifested as Superior Vena Cava Syndrome
Hyein Kang, Su Min Ha, Hye Shin Ahn, Hee Sung Kim, Hee-Jun Kim
J Korean Soc Radiol. 2018;79(4):204-207. doi: 10.3348/jksr.2018.79.4.204.
Reference
-
1. Sasco AJ, Lowenfels AB, Pasker-de Jong P. Review article: epidemiology of male breast cancer. A meta-analysis of published case-control studies and discussion of selected aetiological factors. Int J Cancer. 1993. 53:538–549.
Article2. The Korean Breast Cancer Society. Survival analysis of Korean breast cancer patients diagnosed between 1993 and 2002 in Korea: a nationwide study of the cancer registry. J Breast Cancer. 2006. 9:214–229.
Article3. Donegan WL, Redlich PN. Breast cancer in men. Surg Clin North Am. 1996. 76:343–363.
Article4. Vilcoq JR, Calle R, Ferme F, Veith F. Conservative treatment of axillary adenopathy due to probable subclinical breast cancer. Arch Surg. 1982. 117:1136–1138.
Article5. Baron PL, Moore MP, Kinne DW, Candela FC, Osborne MP, Petrek JA. Occult breast cancer presenting with axillary metastases. Updated management. Arch Surg. 1990. 125:210–214.
Article6. Ellerbroek N, Holmes F, Singletary E, Evans H, Oswald M, McNeese M. Treatment of patients with isolated axillary nodal metastases from an occult primary carcinoma consistent with breast origin. Cancer. 1990. 66:1461–1467.
Article7. Burga AM, Fadare O, Lininger RA, Tavassoli FA. Invasive carcinomas of the male breast: a morphologic study of the distribution of histologic subtypes and metastatic patterns in 778 cases. Virchows Arch. 2006. 449:507–512.
Article8. Copeland EM, McBride CM. Axillary metastases from unknown primary sites. Ann Surg. 1973. 178:25–27.
Article9. Tan PH, Sng IT. Male breast cancer: a retrospective study with immunohistochemical analysis of hormone receptor expression. Pathology. 1997. 29:2–6.
Article10. Giordano SH. A review of the diagnosis and management of male breast cancer. Oncologist. 2005. 10:471–479.
Article11. Gu GL, Wang SL, Wei XM, Ren L, Zou FX. Axillary metastasis as the first manifestation of male breast cancer: a case report. Cases J. 2008. 1:285.
Article12. Chakravarthy A, Kim CR. Post-mastectomy radiation in male breast cancer. Radiother Oncol. 2002. 65:99–103.
Article13. Borgen PI, Senie RT, McKinnon WM, Rosen PP. Carcinoma of the male breast: analysis of prognosis compared with matched female patients. Ann Surg Oncol. 1997. 4:385–388.
Article14. Pentheroudakis G, Lazaridis G, Pavlidis N. Axillary nodal metastases from carcinoma of unknown primary (CUPAx): a systematic review of published evidence. Breast Cancer Res Treat. 2010. 119:1–11.
Article15. Merson M, Andreola S, Galimberti V, Bufalino R, Marchini S, Veronesi U. Breast carcinoma presenting as axillary metastases without evidence of a primary tumor. Cancer. 1992. 70:504–508.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metachronous Contralateral Axillary Lymph Node Metastasis from Invasive Breast Carcinoma: A Case Report with Imaging Findings
- A Recurrence of Ovarian Carcinoma Presenting as Only Axillary Lymphatic Metastasis: A Case Report
- Ipsilateral Breast Tumor Recurrence with Metachronous Contralateral Axillary Lymph Node Metastasis after Breast-Conserving Surgery with Axillary Lymph Node Dissection
- Papillary Thyroid Microcarcinoma Manifesting as Axillary Lymph Node Metastasis: A Case Report
- Ultrasonography for Staging Axillary Lymph Node in Breast Cancer Patients
