Ultrasonographic Characteristics of Mammographically Occult Small Breast Cancer
- Affiliations
-
- 1Department of Radiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
- 2Thanyarak Breast Imaging Center, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
- 3Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. suebwong.chu@mahidol.ac.th
- KMID: 2286461
- DOI: http://doi.org/10.4048/jbc.2012.15.3.344
Abstract
- PURPOSE
To analyze significant ultrasonographic findings of small malignant breast mass (< or =10 mm) which were occult on mammography.
METHODS
The study included 190 small breast masses (< or =10 mm), demonstrated on breast ultrasonography, but not mammography. Histopathology (when the masses were biopsied) or serial breast ultrasonography (for at least 24 months) were used to confirm benign or malignant condition of the masses. Univariate and multivariate logistic regression analysis were used to identify significant characteristic malignant findings on ultrasonography.
RESULTS
Of 190 masses, 46 were cancer, and 144 were benign. On multivariate analyses, irregular shape (odds ratio [OR], 10.4) and not circumscribed margin (OR, 31.6) were significant features to differentiate between benign and malignant breast masses. However, low width/anteroposterior ratio, echogenic halo, hypoechogenecity and posterior acoustic shadow, which were predictors for malignancy in large breast mass, were not documented in small mass.
CONCLUSION
In conclusion, irregular shape and not circumscribed margin detected during ultrasonography were strong predictive signs of malignancy for small malignant breast mass.
Keyword
MeSH Terms
Figure
-
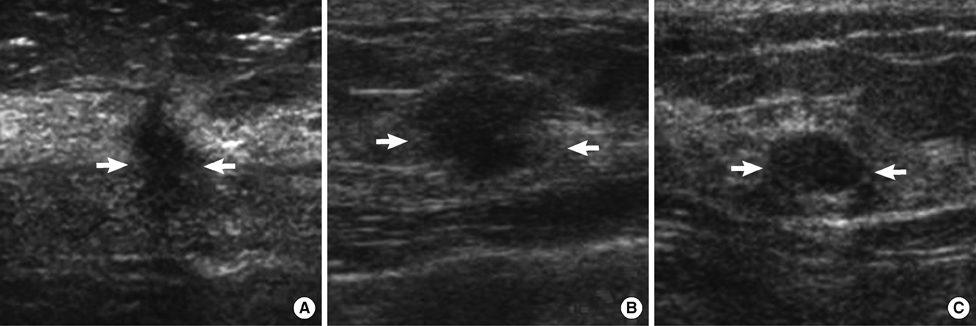
Figure 1 Ultrasonographic findings of malignant and benign breast masses. (A) A mass of invasive ductal carcinoma with irregular shape, not circumscribed margin and hypoechoicity (arrows). (B) A mass of invasive ductal carcinoma with oval shape, not circumscribed margin and hypoechoicity (arrows). (C) A mass, confirmed to be fibroadenoma, showed an oval shape mass, circumscribed margin and hypoechoicity (arrows).
Cited by 2 articles
-
Small Breast Cancer (≤ 5 mm): Ultrasonographic Features and Clinical and Pathological Characteristic
Hye Young Kwon, Eun-Suk Cha, Jee Eun Lee, Jeoung Hyun Kim, Jin Chung
J Korean Soc Radiol. 2019;80(4):728-739. doi: 10.3348/jksr.2019.80.4.728.Breast Cancer Risk Factors in a Defined Population: Weighted Logistic Regression Approach for Rare Events
Najf Zare, Elham Haem, Kamran B. Lankarani, Seyyed Taghi Heydari, Esmat Barooti
J Breast Cancer. 2013;16(2):214-219. doi: 10.4048/jbc.2013.16.2.214.
Reference
-
1. Elmore JG, Armstrong K, Lehman CD, Fletcher SW. Screening for breast cancer. JAMA. 2005. 293:1245–1256.
Article2. Smith RA, Cokkinides V, Brooks D, Saslow D, Brawley OW. Cancer screening in the United States, 2010: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin. 2010. 60:99–119.
Article3. Stojadinovic A, Summers TA, Eberhardt J, Cerussi A, Grundfest W, Peterson CM, et al. Consensus recommendations for advancing breast cancer: risk identification and screening in ethnically diverse younger women. J Cancer. 2011. 2:210–227.
Article4. Chao TC, Chen MF, Wang CS, Jan YY, Hwang TL, Chen SC. Small invasive breast carcinomas in Taiwanese women. Ann Surg Oncol. 2003. 10:740–747.
Article5. Crystal P, Strano SD, Shcharynski S, Koretz MJ. Using sonography to screen women with mammographically dense breasts. AJR Am J Roentgenol. 2003. 181:177–182.
Article6. Corsetti V, Houssami N, Ghirardi M, Ferrari A, Speziani M, Bellarosa S, et al. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer. 2011. 47:1021–1026.
Article7. Muttarak M, Pojchamarnwiputh S, Chaiwun B. Breast carcinomas: why are they missed? Singapore Med J. 2006. 47:851–857.8. Kelly KM, Dean J, Comulada WS, Lee SJ. Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol. 2010. 20:734–742.
Article9. Bassett LW, Ysrael M, Gold RH, Ysrael C. Usefulness of mammography and sonography in women less than 35 years of age. Radiology. 1991. 180:831–835.
Article10. Moy L, Slanetz PJ, Moore R, Satija S, Yeh ED, McCarthy KA, et al. Specificity of mammography and US in the evaluation of a palpable abnormality: retrospective review. Radiology. 2002. 225:176–181.
Article11. Yu PC, Lee YW, Chou FF, Wu SC, Huang CC, Ng SH, et al. Clustered microcalcifications of intermediate concern detected on digital mammography: ultrasound assessment. Breast. 2011. 20:495–500.
Article12. Chen SC, Cheung YC, Su CH, Chen MF, Hwang TL, Hsueh S. Analysis of sonographic features for the differentiation of benign and malignant breast tumors of different sizes. Ultrasound Obstet Gynecol. 2004. 23:188–193.
Article13. Bae MS, Han W, Koo HR, Cho N, Chang JM, Yi A, et al. Characteristics of breast cancers detected by ultrasound screening in women with negative mammograms. Cancer Sci. 2011. 102:1862–1867.
Article14. Stavros AT, Thickman D, Rapp CL, Dennis MA, Parker SH, Sisney GA. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995. 196:123–134.
Article15. Barton MB, Elmore JG, Fletcher SW. Breast symptoms among women enrolled in a health maintenance organization: frequency, evaluation, and outcome. Ann Intern Med. 1999. 130:651–657.
Article16. Chao TC, Lo YF, Chen SC, Chen MF. Prospective sonographic study of 3093 breast tumors. J Ultrasound Med. 1999. 18:363–370.
Article17. Skaane P, Engedal K. Analysis of sonographic features in the differentiation of fibroadenoma and invasive ductal carcinoma. AJR Am J Roentgenol. 1998. 170:109–114.
Article18. Hong AS, Rosen EL, Soo MS, Baker JA. BI-RADS for sonography: positive and negative predictive values of sonographic features. AJR Am J Roentgenol. 2005. 184:1260–1265.
Article19. Paulinelli RR, Freitas-Júnior R, Moreira MA, Moraes VA, Bernardes-Júnior JR, Vidal Cda S, et al. Risk of malignancy in solid breast nodules according to their sonographic features. J Ultrasound Med. 2005. 24:635–641.
Article20. Burnside ES, Hall TJ, Sommer AM, Hesley GK, Sisney GA, Svensson WE, et al. Differentiating benign from malignant solid breast masses with US strain imaging. Radiology. 2007. 245:401–410.
Article21. Rahbar G, Sie AC, Hansen GC, Prince JS, Melany ML, Reynolds HE, et al. Benign versus malignant solid breast masses: US differentiation. Radiology. 1999. 213:889–894.
Article22. Fornage BD, Lorigan JG, Andry E. Fibroadenoma of the breast: sonographic appearance. Radiology. 1989. 172:671–675.
Article23. Baker JA, Kornguth PJ, Soo MS, Walsh R, Mengoni P. Sonography of solid breast lesions: observer variability of lesion description and assessment. AJR Am J Roentgenol. 1999. 172:1621–1625.
Article24. Cole-Beuglet C, Soriano RZ, Kurtz AB, Goldberg BB. Ultrasound analysis of 104 primary breast carcinomas classified according to histopathologic type. Radiology. 1983. 147:191–196.
Article25. Kossoff G. Causes of shadowing in breast sonography. Ultrasound Med Biol. 1988. 14:Suppl 1. 211–215.
Article26. Kwak JY, Kim EK, You JK, Oh KK. Variable breast conditions: comparison of conventional and real-time compound ultrasonography. J Ultrasound Med. 2004. 23:85–96.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum to: Ultrasonographic Characteristics of Mammographically Occult Small Breast Cancer
- Reliability of Breast Ultrasound BI-RADS Final Assessment in Mammographically Negative Patients with Nipple Discharge and Radiologic Predictors of Malignancy
- Small Breast Cancer (≤ 5 mm): Ultrasonographic Features and Clinical and Pathological Characteristics
- Efficacy of Ultrasonography in Breast Cancer Screening
- Characteristics of Clinically Occult Breast Carcinoma
