Recurrent Bilateral Breast Abscess Due to Nontuberculous Mycobacterial Infection
- Affiliations
-
- 1Department of Radiology, Inha University Hospital, Inha University College of Medicine, Incheon, Korea. kimyj@inha.ac.kr
- 2Korea Health Promotion Foundation, Seoul, Korea.
- 3Department of Surgery, Inha University Hospital, Inha University College of Medicine, Incheon, Korea.
- 4Department of Pathology, Inha University Hospital, Inha University College of Medicine, Incheon, Korea.
- KMID: 2286359
- DOI: http://doi.org/10.4048/jbc.2014.17.3.295
Abstract
- Since recurrent bilateral breast infection due to nontuberculous mycobacterium (NTM) is rare, its diagnosis is easily overlooked; in addition, complete recovery is often difficult to achieve. We report a case of recurrent bilateral infection in a 35-year-old woman who had completed treatment for NTM. Although various infectious diseases show similar clinical conditions and imaging findings, recurrences should raise suspicion of NTM infection, and this possibility should be considered in differential diagnoses.
MeSH Terms
Figure
-
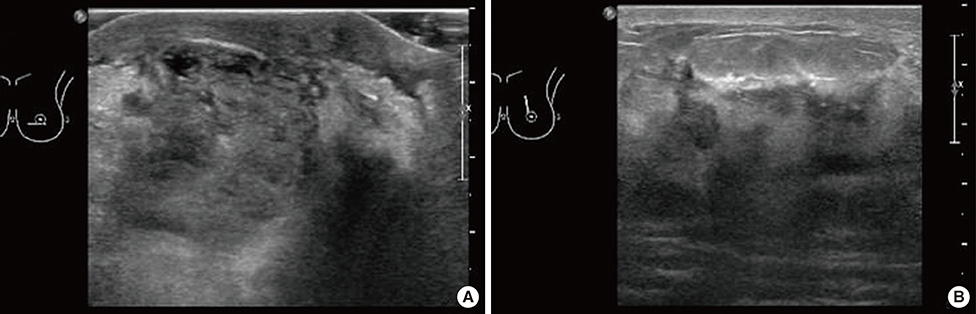
Figure 1 B-mode gray scale ultrasonography of the left breast. (A) Ultrasonogram shows an approximately 2.8 cm ill-defined and partially multilobulating contoured mass with heterogeneous internal echogenicity in the subareolar area. (B) Additional findings of diffuse edematous changes in the left breast, with marked heterogeneous underlying parenchymal echogenicity and skin thickening.
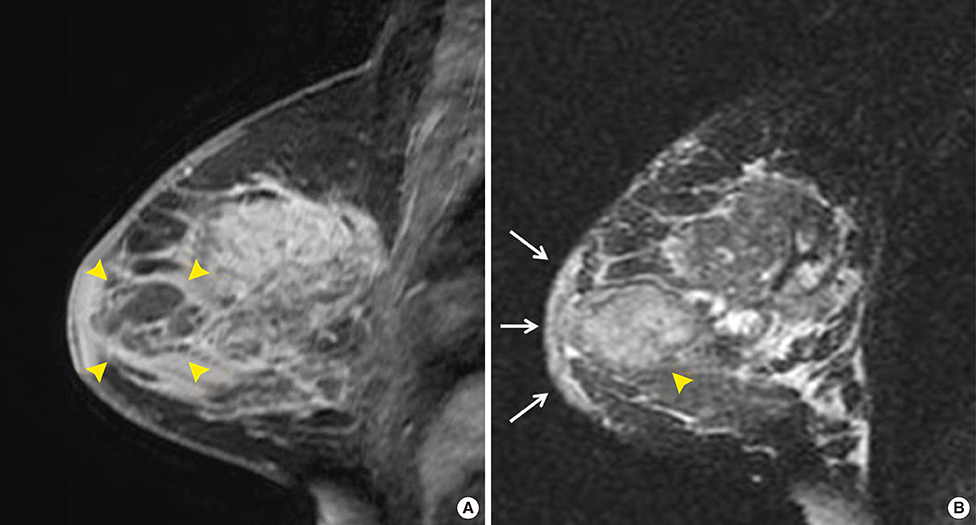
Figure 2 Magnetic resonance imaging: sagittal view of the left breast. (A) Contrast-enhanced magnetic resonance imaging shows an ill-defined and partially multilobular contoured lesion with rim-like enhancement in the subareolar area of the left breast (arrowheads) with additional diffuse parenchymal enhancement. The lesion (arrowheads) visible in the subareolar area correlates to the lesion detected by B-mode gray scale ultrasonography (Figure 1). This lesion appeared to be an abscess consistent with mastitis (1.5-T MR scanner, 3D fat-suppressed T1-weighted Gradient Echo Sequences; contrast injection of 0.2 mL/kg gadodiamide [OmniscanTM; GE Healthcare] was administered by manually followed by a 20-mL saline flush). (B) T2-weighted image showing high signal intensity diffuse edematous changes with skin thickening (arrows) and an ill-defined high signal intensity lesion in the subareolar area (arrowhead), correlated with the lesion with rim-like enhancement.

Figure 3 Histopathologic findings. Histologic sections of the lesion specimen obtained by ultrasound-guided core needle biopsy (A, lower magnified image, ×20; B, higher magnified image, ×100) show inflamed breast tissue with granulomatous reaction on hematoxylin and eosin staining (arrows).
Reference
-
1. Kamal RM, Hamed ST, Salem DS. Classification of inflammatory breast disorders and step by step diagnosis. Breast J. 2009; 15:367–380.
Article2. Chirra A. Nontuberculous Mycobacterium infection of the breast. Proceedings of UCLA Healthcare. Accessed December 4th, 2013. Available from: http://www.med.ucla.edu/modules/wfsection/article.php?articleid=567.3. Macadam SA, Mehling BM, Fanning A, Dufton JA, Kowalewska-Grochowska KT, Lennox P, et al. Nontuberculous mycobacterial breast implant infections. Plast Reconstr Surg. 2007; 119:337–344.
Article4. Abdelhadi MS, Bukharie HA. Breast infections in non-lactating women. J Family Community Med. 2005; 12:133–137.5. Tewari M, Shukla HS. Breast tuberculosis: diagnosis, clinical features & management. Indian J Med Res. 2005; 122:103–110.6. Coney PM, Thrush S. Cutaneous Mycobacterium fortuitum complicating breast reconstruction. J Plast Reconstr Aesthet Surg. 2007; 60:1162–1163.
Article7. Vinh DC, Rendina A, Turner R, Embil JM. Breast implant infection with Mycobacterium fortuitum group: report of case and review. J Infect. 2006; 52:e63–e67.
Article8. Rimmer J, Hamilton S, Gault D. Recurrent mycobacterial breast abscesses complicating reconstruction. Br J Plast Surg. 2004; 57:676–678.
Article9. Haiavy J, Tobin H. Mycobacterium fortuitum infection in prosthetic breast implants. Plast Reconstr Surg. 2002; 109:2124–2128.
Article10. Medical Section of the American Lung Association. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Am J Respir Crit Care Med. 1997; 156:S1–S25.11. Betal D, Macneill FA. Chronic breast abscess due to Mycobacterium fortuitum: a case report. J Med Case Rep. 2011; 5:188.
Article12. Cooke FJ, Friedland JS. Spontaneous breast abscess due to Mycobacterium fortuitum. Clin Infect Dis. 1998; 26:760–761.
Article13. Lewis CG, Wells MK, Jennings WC. Mycobacterium fortuitum breast infection following nipple-piercing, mimicking carcinoma. Breast J. 2004; 10:363–365.
Article14. Bengualid V, Singh V, Singh H, Berger J. Mycobacterium fortuitum and anaerobic breast abscess following nipple piercing: case presentation and review of the literature. J Adolesc Health. 2008; 42:530–532.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breast Abscess due to Mycobacterium Fortuitum: A Case Report
- Huge Abscess due to Mycobacterium Abscessus Infection after Breast Augmentation
- Chronic Large Non Healing Ulcer: Non-Tuberculous Mycobacterial Infection of the Laryngopharynx
- Nontuberculous Mycobacterial Tenosynovitis in the Hand: Two Case Reports with the MR Imaging Findings
- Nontuberculous Mycobacterial Infection after Breast Reconstruction with an Implant: A Case Report
