Radiographic Detection of Osteoporotic Vertebral Fracture without Collapse
- Affiliations
-
- 1Department of Orthopedic Surgery, School of Medicine, Wonkwang University Hospital, Iksan, Korea. oschae68@hanmail.net
- 2Department of Radiology, School of Medicine, Wonkwang University Hospital, Iksan, Korea.
- KMID: 2286299
- DOI: http://doi.org/10.11005/jbm.2013.20.2.89
Abstract
- BACKGROUND
On retrospective basis, we investigated the detection of osteoporotic vertebral fractures (OVFs) without radiologic collapse using a modified Yoshida's classification, which was designed by the authors.
METHODS
We observed 82 cases in 76 patients with confirmed OVFs without collapse at the thoracolumbar junction. The following factors were measured: age, gender, body mass index (BMI, kg/m2), bone mineral density (BMD, mg/cm3), type of a modified Yoshida's classification. The correct diagnosis rate for the presence and location of OVFs and the correct diagnosis rate according to the morphological type by a modified Yoshida's classification of the OVFs were analyzed.
RESULTS
The mean BMI was 21.2; mean BMD, 44.1; and T-score, -4.4. As for the four subtypes of anterior cortical morphological change, there were 14 cases of the protruding type, 12 cases of the indented type, 5 cases of the disrupted type and 8 cases of the prow type. As for the three subtypes of endplate depression, there were 20 cases of upper endplate depression, 12 cases of lower endplate depression and 11 cases of endplate slippage type. According to the examiners, there was a significant difference between being informed before and after the modified Yoshida's classification. For the relationship of examiners and the type of fracture, there was a significant difference between being informed before and after the modified Yoshida's classification, particularly in the protruding type and the upper plate type.
CONCLUSIONS
A modified Yoshida's classification can be helpful for the diagnosis of OVFs without radiologic collapse in a simple radiograph.
Keyword
Figure
-

Fig. 1 A modified Yoshida classified into two types and seven subtypes. Anterior cortical morphological change types: Protrusion type, the anterior bony cortex disrupted protrudes anteriorly; indented type, the anterior bony cortex disrupted indents posteriorly; disrupted type, the anterior bony cortex disrupted with no displacement; prow type, the anterior bony cortex disrupted mixed of anterior and posterior. Endplate compression types: upper endplate depression type, the center of the upper endplate disrupted and depression; lower endplate depression type, the center of the lower endplate disrupted and depression; endplate slippage type, the anterior edge of the endplate disrupted anteriorly.
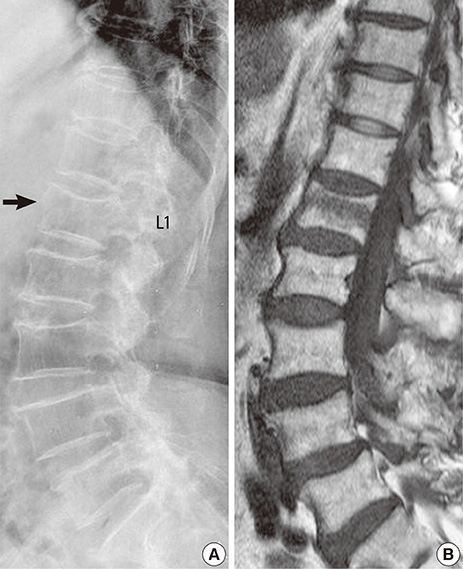
Fig. 2 An 87-year-old woman with occult osteoporotic vertebral fractures of L1 (A), confirmed by magnetic resonance imaging (B). L1 has a change of anterior cortex morphology (protruding type of modified Yoshida's classification) (arrow).

Fig. 3 A 92-year-old woman with occult osteoporotic vertebral fractures of L1 (A), confirmed by MRI (B). L1 has a change of endplate morphology (upper endplate slippage type of modified Yoshida's classification) (arrow).
Reference
-
1. Bliuc D, Nguyen ND, Milch VE, et al. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009; 301:513–521.
Article2. O'Neill TW, Cockerill W, Matthis C, et al. Back pain, disability, and radiographic vertebral fracture in European women: a prospective study. Osteoporos Int. 2004; 15:760–765.3. Grados F, Fechtenbaum J, Flipon E, et al. Radiographic methods for evaluating osteoporotic vertebral fractures. Joint Bone Spine. 2009; 76:241–247.
Article4. Genant HK, Jergas M. Assessment of prevalent and incident vertebral fractures in osteoporosis research. Osteoporos Int. 2003; 14:Suppl 3. S43–S55.
Article5. Lenchik L, Rogers LF, Delmas PD, et al. Diagnosis of osteoporotic vertebral fractures: importance of recognition and description by radiologists. AJR Am J Roentgenol. 2004; 183:949–958.
Article6. Grigoryan M, Guermazi A, Roemer FW, et al. Recognizing and reporting osteoporotic vertebral fractures. Eur Spine J. 2003; 12:Suppl 2. S104–S112.
Article7. Delmas PD, van de Langerijt L, Watts NB, et al. Underdiagnosis of vertebral fractures is a worldwide problem: the IMPACT study. J Bone Miner Res. 2005; 20:557–563.
Article8. Williams AL, Al-Busaidi A, Sparrow PJ, et al. Under-reporting of osteoporotic vertebral fractures on computed tomography. Eur J Radiol. 2009; 69:179–183.
Article9. Fechtenbaum J, Cropet C, Kolta S, et al. Reporting of vertebral fractures on spine X-rays. Osteoporos Int. 2005; 16:1823–1826.
Article10. Fink HA, Milavetz DL, Palermo L, et al. What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J Bone Miner Res. 2005; 20:1216–1222.
Article11. Pham T, Azulay-Parrado J, Champsaur P, et al. "Occult" osteoporotic vertebral fractures: vertebral body fractures without radiologic collapse. Spine (Phila Pa 1976). 2005; 30:2430–2435.12. Ito Z, Harada A, Matsui Y, et al. Can you diagnose for vertebral fracture correctly by plain X-ray? Osteoporos Int. 2006; 17:1584–1591.
Article13. Mao H, Zou J, Geng D, et al. Osteoporotic vertebral fractures without compression: key factors of diagnosis and initial outcome of treatment with cement augmentation. Neuroradiology. 2012; 54:1137–1143.
Article14. Kanchiku T, Taguchi T, Kawai S. Magnetic resonance imaging diagnosis and new classification of the osteoporotic vertebral fracture. J Orthop Sci. 2003; 8:463–466.
Article15. Chae SU, Kim GD. Radiographic diagnosis of the osteoporotic vertebral fractures. Osteoporosis. 2013; 11:59–65.16. Guglielmi G, Diacinti D, van Kuijk C, et al. Vertebral morphometry: current methods and recent advances. Eur Radiol. 2008; 18:1484–1496.
Article17. Bennett DL, Post RD. The role of the radiologist when encountering osteoporosis in women. AJR Am J Roentgenol. 2011; 196:331–337.
Article18. Kim N, Rowe BH, Raymond G, et al. Underreporting of vertebral fractures on routine chest radiography. AJR Am J Roentgenol. 2004; 182:297–300.
Article19. Majumdar SR, Kim N, Colman I, et al. Incidental vertebral fractures discovered with chest radiography in the emergency department: prevalence, recognition, and osteoporosis management in a cohort of elderly patients. Arch Intern Med. 2005; 165:905–909.
Article20. Nakano T, Ochi R, Miyazono K, et al. Diagnosis precision of MRI for fresh osteoporotic vertebral body fracture and a diagnosis by follow-up roentgenogram (in Japanese). Osteoporos Jpn. 2004; 12:89–90.21. Tanigawa N, Komemushi A, Kariya S, et al. Percutaneous vertebroplasty: relationship between vertebral body bone marrow edema pattern on MR images and initial clinical response. Radiology. 2006; 239:195–200.
Article22. Yamato M, Nishimura G, Kuramochi E, et al. MR appearance at different ages of osteoporotic compression fractures of the vertebrae. Radiat Med. 1998; 16:329–334.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiographic Diagnosis of the Osteoporotic Vertebral Fractures
- Prediction of Subsequent Vertebral Collapse after Osteoporotic Thoracolumbar Vertebral Fractures
- The Diagnosis of Osteoporotic Occult Vertebral Fracture and Vertebroplasty
- The Effect of Disc Degeneration in Osteoporotic Vertebral Fracture
- Posttraumatic Delayed Vertebral Collapse : Kummell's Disease
